REVIEW ARTICLE
NURSING ASSISTANCE TO ONCOLOGICAL
PATIENTS WHO CONTRACTED COVID-19 DURING TREATMENT
ASISTENCIA DE
ENFERMERÍA A PACIENTES ONCOLÓGICOS QUE CONTRAYERON COVID-19 DURANTE EL
TRATAMIENTO
ASSISTÊNCIA DE ENFERMAGEM À PACIENTES
ONCOLÓGICOS QUE CONTRAÍRAM COVID-19 DURANTE O TRATAMENTO
https://doi.org/10.31011/reaid-2023-v.97-n.2-art.1581
1Geovana Maria de Oliveira
2Poliana Martins Ferreira
3Namie Okino Sawada
1Universidade Federal de Alfenas, Alfenas,
Brasil, ORCID: https://orcid.org/0000-0002-1415-7389
2Universidade Federal de Alfenas, Alfenas,
Brasil, ORCID: https://orcid.org/0000-0002-9780-8633
3Universidade Federal de Alfenas, Alfenas,
Brasil, ORCID: https://orcid.org/0000-0002-1874-3481
Corresponding author
Geovana Maria de Oliveira
Alcino Alves de Barros, Bairro: Jardim Alvorada, N°
43, CEP: 37.160-000, Campos Gerais MG – Brazil. +55 (35) 98708-5319, E-mail:
geovana.oliveira@sou.unifal-mg.edu.br
Submission: 16-11-2022
Approval: 09-05-2023
Sponsorship and Acknowledgment: CNPq,
thanks for funding and support for carrying out the research
ABSTRACT
Objective: To identify in
the national and international literature scientific evidence on nursing care
provided to people undergoing cancer treatment who contracted Covid-19. Method:
Integrative Review where the guiding question was based on the PICO strategy.
LILACS, PubMed, Web of Science, Embase, CINAHL databases were used. As
inclusion criteria: adult cancer patients (aged 18 and over), published from
January 2020 to December 2021 in English, Portuguese, and Spanish. The
controlled descriptors will be used: Coronavirus; Nursing care; Cancer;
Coronavirus infections; Nursing; Oncology; Pandemic; Covid-19; Chemotherapy;
Oncology Nursing; Results: The corpus of this IR consisted of 8
articles, which met the inclusion criteria with evidence levels II and IV. The
synthesis of knowledge pointed to two categories 1- Postponement of treatment
and 2 - Technologies. Final considerations: Treatment was interrupted
during the pandemic and technological means such as telehealth care and phone
calls were used to maintain nursing care. In addition, it was possible to
identify gaps such as: few investigations available in full with a deepening on
the subject and with strategies to subsidize nursing care and clinical practice
and the studies were mostly of low level of evidence.
Keywords: Nursing Care;
Neoplasms; Coronavirus Infections; Covid-19; Oncology Nursing.
RESUMEN
Objetivo: Identificar en la
literatura nacional e internacional evidencias científicas sobre los cuidados
de enfermería brindados a personas en tratamiento oncológico que contrajeron
Covid-19. Método: Revisión Integrativa donde la pregunta orientadora se
basó en la estrategia PICO. Se utilizaron las bases de datos LILACS, PubMed,
Web of Science, Embase, CINAHL. Como criterios de inclusión: pacientes
oncológicos adultos (mayores de 18 años), publicados de enero de 2020 a diciembre
de 2021 en inglés, portugués y español. Se utilizarán los descriptores
controlados: Coronavirus; Cuidado de enfermera; Cáncer; infecciones por
coronavirus; Enfermería; Oncología; Pandemia; COVID-19; Quimioterapia;
Enfermería Oncológica; Resultados: El corpus de este RI estuvo compuesto
por 8 artículos, que cumplieron los criterios de inclusión con niveles de
evidencia II y IV. La síntesis de conocimientos apuntó dos categorías 1-
Aplazamiento del tratamiento y 2- Tecnologías. Consideraciones finales:
El tratamiento fue interrumpido durante la pandemia y se utilizaron medios
tecnológicos como la atención de telesalud y llamadas telefónicas para mantener
los cuidados de enfermería. Además, fue posible identificar vacíos como: pocas
investigaciones disponibles en su totalidad con una profundización sobre el
tema y con estrategias para subsidiar el cuidado y la práctica clínica de
enfermería y los estudios en su mayoría fueron de bajo nivel de evidencia.
Palabras clave: Atención
de Enfermería; Neoplasias; Infecciones por Coronavirus; COVID-19; Enfermería
Oncológica.
RESUMO
Resumo: Objetivo: Identificar na literatura nacional e internacional
evidências científicas sobre assistência de enfermagem prestada às pessoas em
tratamento oncológico, que contraíram Covid-19. Método: Revisão
Integrativa onde a questão norteadora foi baseada na estratégia PICO.
Utilizou-se das bases de dados LILACS, PubMed, Web of Science, Embase, CINAHL.
Como critérios de inclusão: pacientes oncológicos adultos (maiores e iguais a
18 anos), publicados no período de janeiro de 2020 a dezembro de 2021 nos
idiomas inglês, português e espanhol. Foram utilizados os descritores
controlados: Coronavírus; Cuidados de Enfermagem; Câncer; Infecções por
Coronavírus; Enfermagem; Oncologia; Pandemia; Covid-19; Quimioterapia;
Enfermagem Oncológica; Resultados: O corpus dessa RI foram 8 artigos,
que atenderam aos critérios de inclusão com níveis de evidências II e IV. A
síntese do conhecimento apontou para duas categorias 1- Adiamento do tratamento
e 2 – Tecnologias. Considerações finais: Houve interrupção do tratamento
durante a pandemia e foram utilizados meios tecnológicos como atendimento de
tele saúde e chamadas telefônicas para manter a assistência de enfermagem.
Ademais, foi possível identificar lacunas como: poucas investigações
disponíveis na íntegra com um aprofundamento no tema e com estratégias para
subsidiar a assistência de enfermagem e a prática clínica e os estudos foram na
maioria de nível de evidência baixo.
Palavras-chave:
Cuidados de Enfermagem; Neoplasias; Infecções por Coronavírus; Covid-19;
Enfermagem Oncológica.
INTRODUCTION
According to the National Cancer Institute (INCA),
cancer is a term that covers more than 100 malignant diseases that have in
common the disordered growth of cells. These cells tend to divide rapidly and
group together to form tumors, in an uncontrollable and aggressive manner. It
is characterized by invading adjacent tissues through the speed of
multiplication of the cells or distant organs through metastases.¹
During the evolution of normal cells to the neoplastic
state, the so-called "hallmarks of cancer" occur, where these cells
share characteristics that ensure resistance to apoptosis, replicating
immortality, activation of invasion and metastasis, inflammation, and
reprogramming of metabolism, among others. This occurs due to changes in the
structure of the cells, from mutations caused by external (cigarette smoking,
eating habits, alcohol consumption, exposure to radiation, viruses, among
others) or internal factors (hormones, compromised immune system, or genetic
predisposition).2,3
According to epidemiology, cancer is characterized as
the second leading cause of death worldwide. In the year 2018, 9.6 million
deaths from the disease were estimated. In Brazil, between 2020 and 2022,
625,000 new cases are estimated for each year and for 2025, more than 20
million new cases are expected.4
According to INCA, in Brazil in 2020, the incidence
according to the primary location of the tumor in men stood out in the prostate
with 29.2% and in women in the breast with 29.7%. As for mortality, according
to the primary location of the tumor, in men the trachea, bronchi and lungs
stood out with 13.8% and in women the breast with 16.4%.5.
Allied to this is the new coronavirus that causes
Covid-19, which is an acute infectious respiratory disease caused by the
SARS-CoV-2 virus of the Coronaviridae family. The symptoms can be mild (fever,
tiredness, and cough) or more severe (high fever, pneumonia, and dyspnea).
There are also asymptomatic carriers of great epidemiological importance
because they are potential transmitters.6
According to epidemiological data compiled by the
Center for Systems Science and Engineering at Johns Hopkins University, more
than 402 million cases have been reported worldwide, with 5.7 million deaths
being reported by March 2022. Brazil is the country with the second-highest
number of infections and deaths, with 29,368,776 cases and 655,078 deaths
reported by March 2022.7,8
Also, it is worth noting that one of the main risk
factors for COVID-19 is immunosuppressed people (low immune responses) with
chronic diseases. They are more susceptible to developing more intense symptoms
because certain health conditions and comorbidities can influence the body's
immune response. Because of this, they deserve special attention during a
pandemic.9
It should be noted, however, that cancer patients are
a high-risk group in the pandemic of COVID-19 because their immune system is
compromised, making them vulnerable to infection. Furthermore, because they
already have an underlying disease, they have an increased risk of developing
serious complications if infected with the virus.10
According to Coronavirus Disease, 2021, in addition to
low immunity triggered by treatment, oncology patients are prone to COVID-19
infection due to the need to attend hospitals for access to cancer diagnosis,
treatment and follow-up.8
According to epidemiological data, 20% of COVID-19
cases in cancer patients were due to in-hospital infection. And within a sample
of 181 followed-up patients admitted to INCA during a certain time, 60 died
because of the new coronavirus. Furthermore, during the study, it was also
found that the evolution of the virus in tumor patients is faster compared to
healthy health professionals. Regarding death by type of cancer, lung cancer
stands out in first place, followed by breast cancer, followed by malignant
myeloma.11
Nursing participates directly in the health-disease
process, with actions linked to the patient and family members since the
diagnosis, treatment, and prognosis, following each stage. In this context, it
has a fundamental role in health care, developing new techniques and strategies
that can minimize the impacts generated by the pandemic in oncologic treatment,
so that treatment does not become a risk due to the high virulence of
SARS-CoV-2 and to provide greater attention to the early intervention of
symptoms in infected patients.10
Therefore, the aim of this study is to identify in the
national and international literature scientific evidence on nursing care
provided to people in cancer treatment, who contracted COVID-19.
METHODS
The research method used in this study was an
Integrative Review, based on EBP, which allows for the synthesis of knowledge
through a systematic and rigorous process. We opted for the proposal addressed
by Mendes, Silveira and Galvão (2019), which goes through six steps: 1)
Preparation of the review question; 2) Search and selection of primary studies;
3) Extraction of data from the studies; 4) Critical appraisal of the primary
studies included in the review; 5) Synthesis of the review results and 6)
Presentation of the method.12
First
Stage: Preparation of the Review Question:
The guiding question of this present study was formulated
according to the PICO strategy, where P=oncology patients in treatment, I=
COVID- 19 C=not applicable, O=Nursing care, thus the question of this IR is:
How has been the nursing care provided to cancer patients who contracted COVID-
19 during treatment?
Second phase: Search and selection of
primary studies:
Therefore, as inclusion criteria, the following were
defined: Primary studies that address the theme Nursing care in cancer patients
who contracted the COVID-19 virus during treatment, in adult patients (greater
than and equal to 18 years old), published in the period from January 2020 to
December 2021 in the languages, Portuguese, English and Spanish indexed in the
databases:
- LILACS (Latin
American and Caribbean Health Science Literature Database), site: http://lilacs.bvsalud.org/.
- Pub Med (Public
Medline or Publisher Medline), site: https://www.ncbi.nlm.nih.gov/pubmed/.
- WEB OF SCIENCE,
site: apps-webofknowledge.ez37.periodicos.capes.gov.br.
- EMBASE, site: https://www.embase.com/landing?status=grey
- CINAHL:
https://www.sciencedirect.com/topics/nursing-and-health-professions/cinahl
And
the exclusion criteria were letters, comments, editorials, opinion articles,
and review articles.
For the search of the articles, the Descriptors in
Health Sciences (DECS) described below were used:
Coronavirus; Nursing Care; Cancer; Coronavirus
Infections; Nursing; Oncology; Pandemic; Covid-19; Chemotherapy; Oncology
Nursing.
And the Medical Subject Headings (MESH) descriptors:
Coronavirus; Nursing care; Cancer; Coronavirus infections; Nursing; Oncology;
Pandemic; Covid-19; Chemotherapy; Oncology Nursing.
The
Boolean operator represented by the AND connector was used and all descriptors,
crossings were made with all descriptors and every time that more than 200
results came in, one more descriptor was added.
Third phase: Data extraction from the
primary studies:
The Endnote software was used to organize the articles
resulting from the search, excluding duplicates. After that, it was exported to
the Rayyan software, which contains variables such as title of the article,
journal, authors, year, country of publication, and language, for selection of
the articles from readings by titles and abstracts and after that, selection by
reading in full. The analysis of the inclusion of the articles was made by two
reviewers in a blinded fashion.
Fourth phase:
Critical appraisal of the primary studies:
To perform this
step, an instrument constructed by the authors was used and level of evidence
according to Melhink & Fineout 2019, which advocates levels according to
the research question and design for Intervention/Treatment or
Diagnostic/Testing studies. Apparent and content validation of this instrument
was performed by 3 expert judges.13
Fifth
phase: Synthesis of the review results
In this next step, the discussion of results is
performed, where the reviewer can make a critical evaluation of the studies by
comparing them with the theoretical knowledge, identifying gaps that allow the
identification of factors that affect nursing policy and care. From this, it is
possible to point out pertinent suggestions for future research on improving
health care.12
Sixth phase: Presentation
of the review
This phase is the last step in the development of an
integrative review, and simply consists of a document containing the
description of the steps taken by the reviewer and the main results obtained
from the included articles. It is significant, as it produces an impact
generated by the accumulation of knowledge on the theme and the dissemination
of results that contemplate health professionals in different places and at
different times, keeping them updated and facilitating changes in clinical
practice because of the research.12
RESULTS
Figure 1 - Flowchart
prepared according to the Identification of studies through database,
selection, eligibility, and inclusion of studies in the Integrative Review
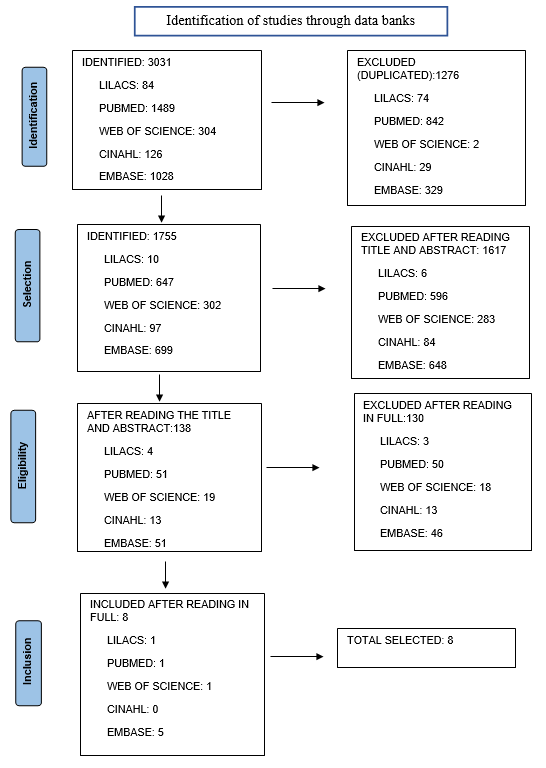
Source: Elaborated by the author - according to Page 14
Chart1
- Description of the studies included in the
Integrative Review according to author(s), titles, and database where they were
located
|
No.
|
AUTHOR(S)
|
TITLE
|
DATABASES
|
|
1
|
Cavanna
L. et al.
|
Prevalence
of COVID-19 infecion in asymptomatic câncer patients in a district with high
prevalence of SARS-CoV-2 in Italy.15
|
WEB
OF SCIENCE
|
|
2
|
Elkin
E. et al.
|
A
covid-19 screening tool for oncology telefone triage.16
|
EMBASE
|
|
3
|
Ferrua
M. et al.
|
Nurse
navigators’ letemonitoring for câncer patients with COVID-19: a French case
study.17
|
PUBMED
|
|
4
|
Miaskowshi
C.
|
Oncology
patients’ perceptions of and experiences with COVID-19.18
|
EMBASE
|
|
5
|
Pritchett
JC. et al.
|
Association
of a remote patient monitoring (RPM) program with reduced hospitalizations in
câncer patients with COVID-19.19
|
EMBASE
|
|
6
|
Sampaio
SGSM. et al.
|
Evaluation
of the criteria adopted to identify suspected cases of COVID-19 in the
Emergency Department Service of a Referral
Palliative Oncology Care Unit.20
|
EMBASE
|
|
7
|
Santiago
FB, Silva ALA.
|
First
case of COVID-19 in an Oncological Palliative Care Unit: Experience Report.21
|
LILACS
|
|
8
|
Strang
P. et al.
|
Dying
from cancer with COVID-19: age, sex.22
|
EMBASE
|
Source: Elaborated by the author
Chart 2
- Description
of the studies included in the Integrative Review according to:
journals,
year of publication, country of origin, type of study and level of evidence
|
No.
|
Journal
|
Year of publication
|
Country of origin
|
Type of study
|
Level of evidence
|
|
1
|
Cureus
|
2021
|
Brazil
|
Retrospective analytical
|
II
|
|
2
|
Supportive Care in Cancer
|
2020
|
United States
|
Methodological
|
IV
|
|
3
|
Supportive Care in Cancer
|
2021
|
France
|
Cross-sectional
|
IV
|
|
4
|
Supportive Care in Cancer
|
2020
|
United States
|
Cross-sectional
|
IV
|
|
5
|
JCO Oncology Practice
|
2021
|
United States
|
Cross-sectional
|
IV
|
|
6
|
American Journal of Hospice & Palliative
Medicine
|
2021
|
Brazil
|
Cross-sectional
|
IV
|
|
7
|
Enfermagem foco
|
2020
|
Brazil
|
Experience report, descriptive
|
IV
|
|
8
|
Acta Oncologia
|
2021
|
Sweden
|
Descriptive and retrospective
|
IV
|
Chart
3 - Description of the studies included in the
Integrative Review according to: sample characteristics and main results.
|
No.
|
Sample characteristics
|
Main results
|
|
1
|
In a 2-month period in the outpatient clinic of a
general hospital, 260 cancer patients were tested for Covid-19, with 10
patients testing positive.15
|
Cancer treatments are being postponed due to
contamination by sars-cov-2. This is configured in the limitation of the
assistance provided to cancer patients, along with the continuity of
treatment, which may constitute a risk to the life of this population.15
|
|
2
|
Cancer patients from an Integrated Cancer Center,
tested by a screening tool to identify possible symptoms of covid-19.16
|
A telephone screening feature covering
cancer-related questions and covid-19-related symptoms has been implemented,
so that they can refer affected patients and appropriate treatments, without
affecting oncology treatment. Nursing care is limited to phone calls or care
regarding prevention of covid-19.16
|
|
3
|
Data were collected from 130 cancer patients with
COVID-19 diagnosed from March 23 to June 5, 2020.
(median age: 59 years, female).17
|
Using a system called CAPRI-COVID that keeps
COVID-19 patients at home as much as possible while
remotely monitor the daily evolution of related
illnesses such as symptoms to limit irrelevant hospital visits and anticipate
hospital visits when necessary. In addition, RNs supervise the discharge of
patients from an inpatient unit to their homes with primary care providers to
promote continuity of care. Symptom monitoring was performed on patients via
telephone interaction (with RNs) or via CAPRI cell phone app. This method is
justified in the safest way for providers to continue care.17
|
|
4
|
Sample of 174 cancer patients, age > 18 years,
12.2% tested positive for covid-19 and 0.6% were hospitalized for covid-19.18
|
Health professionals are finding it difficult to
understand and differentiate cancer symptoms from covid symptoms, so that
they can follow the evolution of patients through telehealth and provide the
necessary assistance. Thus, it is important that these professionals study
the difference between these two conditions and efficient methods of
assistance.18
|
|
5
|
Adult patients receiving targeted cancer therapy or
in recent remission on active surveillance with SARS-CoV-2 infection
confirmed by polymerase chain reaction between March 18 and July 31, 2020.19
|
The use of a new RPM program and
centralized virtual care team, associated with a
significant reduction in hospital admission rate and lower
overall utilization of acute care resources among
cancer patients with COVID-19. Throughout the COVID-19 pandemic, innovative
care delivery methods have proven
to be essential to ensure continuous care for many
of our vulnerable populations, as due to the high transmission rate of the
virus nursing care is limited.19
|
|
6
|
All patients admitted to an oncology palliative care
unit and emergency department between April and June 2020.20
|
Nurses have used technology to maintain contact
between the patient and family members during the last time of life. This
helps the patient to face this process with less impact and aids in the care
process provided by nurses.20
|
|
7
|
First patient with positive result for COVID 19 in
the oncology palliative care unit and Nursing team of a Federal Institute of
reference for palliative care, in the city of Rio de Janeiro.21
|
Technology is being used to reduce psychic symptoms
(pain, suffering and anguish), since due to the pandemic patients cannot be
in contact with family and friends and furthermore, nursing care becomes
limited, increasing the patient's suffering.21
|
|
8
|
All cancer patients who died during March-May 2020
in the Stockholm region, n ¼ 1467 of whom 278 died with a diagnosis of
COVID-19, compared to deaths in 2016-2019.22
|
Patients with covid-19 could not
palliative care (this issue has an impact on care)
due to the
impact on care) due to the pandemic, as they have
experienced
several changes of location including emergency
care, hospital admissions and hospital wards which causes discomfort and
suffering; Studies show that patients who go through palliative care
had fewer acute admissions and hospital deaths.22
|
Source: Elaborated by the author
Chart
4 - Organization of the studies according to:
categories, subcategories and number of articles.
|
Categories
|
Subcategories
|
No.
of articles
|
%
|
|
Treatment
postponement
|
|
1
|
12.5
|
|
Technology
|
Telehealth
|
5
|
62.5
|
|
|
Telephone
Monitoring
|
2
|
25
|
|
TOTAL
|
|
11
|
100
|
Source: Elaborated by the author
DISCUSSION
According to the category, postponement of treatment,
cited by 1 (12.5%) article, it is possible to identify that facing the high
transmission rate of Sars-CoV-2 health professionals chose to interrupt the
cancer treatment of infected patients to maintain the safety of other patients,
reducing the flow inside hospitals and using these spaces to receive severe
patients infected by the virus. In addition, the lack of supplies has
negatively influenced the health of oncology patients who need drugs for cancer
control, and for COVID-19 control for infected people. 23
The interruption in treatment is distressing for the
health and well-being of these patients, who need treatment to control and/or
fight cancer along with its symptoms. Parallel to this, there was also the
interruption of diagnostic services in this period, which may bring as a
consequence, a higher incidence of discoveries of malignant tumors in advanced
stages, with impact on prognosis and survival time of patients.23
According to the Technology category, addressed by 7
(87.5%) studies, it is possible to identify issues related to physical and
emotional well-being. In this context, technology contributes to the continuity
of treatment, which can occur at home, guided by the professional through a
telephone call or video call. It is also possible to perform the triage process
of this patient, through questions for monitoring the symptoms, helping the
professional to help effectively and, if necessary, referring him/her to a
specialized center.24
The telehealth subcategory, addressed by 5 (62.5%)
articles, has been very efficient to control symptoms, being possible to
differentiate the symptoms caused by cancer and its treatment, from the
symptoms caused by Covid-19. In addition, this system contributes to patient
follow-up, bringing the patient closer to the oncology professional so that no
complications occur.24
Furthermore, 2 (25%) articles mention the subcategory
telephone monitoring, which in addition to bringing the patient closer to the
professional, can be effective in bringing the patient closer to family
members, in cases of hospitalization. It is noteworthy the importance that this
method brings in the continuity of treatment and control of symptoms, and for
the emotional health of patients, especially those in palliative care, reducing
stress, anxiety, and other psychological changes, which can intensify during
social isolation.24
Moreover,
the knowledge that cancer patients are more susceptible to contracting the
virus and developing severe sequels, amplifies the feelings of anxiety,
boredom, and fear, generated by the social isolation necessary for people who
have contracted COVID-19. Such feelings affect the quality of life of
individuals and can cause changes in sleep patterns, changes in physical,
occupational, cognitive, and social functioning.23
FINAL CONSIDERATIONS
The Integrative Review is one of the most used methods
in nursing because it has results systematically, obtained from reliable and
relevant databases, and selected through reading in twice, by two independent
reviewers. It is ordered, by the extraction of data through organized
instruments. And comprehensive, by the junction of several studies that end up
in a final document. This becomes an ally to nurses who have little time to
study all the scientific knowledge available, making research results more
accessible, since in a single IR the reader has access to several studies
conducted.
After
analyzing the studies selected for this Integrative Review, it is concluded
that COVID-19 has had a significant impact on cancer treatment. In some cases,
there was interruption of treatment, in other cases, technological means were
used as telehealth care and phone calls to maintain nursing care to patients
who contracted the virus during treatment, to ensure a qualified care and free
of damage.
One
of the most used ways by the professionals was telehealth care, with which it
is possible to maintain oncology treatment and monitor COVID-19 symptoms.
Moreover, with this method employed, it is possible to bring the patient closer
to the nurse and family members, thus minimizing the emotional impact caused by
social isolation, especially to patients in palliative care in their last time
of life.
Finally, regarding the design of the studies, there is
a predominance of cross-sectional studies, which have advantages such as cheap,
simple, fast, no one is exposed to a causal agent due to the study, or denied a
therapy of potential benefit and are useful for long-term diseases. Most of
them are classified with levels of evidence IV, in other words, they have low
level of evidence for clinical practice, and are characterized as low clinical
recommendation.
Given the presentation of this Integrative Review,
which aimed to assess how has been the nursing care for cancer patients who
contracted the COVID-19 virus during treatment, it raised the following
limitations: few investigations available in full of a deepening of the subject
and with strategies to support nursing care and clinical practice and many
studies with low level of evidence.
This study allows the gathering and synthesizing of
research results contributing to Evidence-Based Practice (EBP), allowing the
nursing professional to have access to a synthesis of multiple published
studies, providing support for decision-making and improving clinical practice.
REFERENCES
1.
Instituto Nacional de Câncer
(BR). Câncer: O que é câncer? [Internet]. Rio de Janeiro: INCA; 2022 [citado
2022 Maio 06]. Disponível em: https://www.inca.gov.br/o-que-e-câncer.
2.
Nagy A, Munkácsy G, Gyôrffy B. Análise de sobrevivência ao
câncer de gênes característicos do câncer. Representante Científico [Internet]. 2021 [citado 2022 Mar 14]; 11(6047). Disponível em:
https://www.nature.com/articles/s41598-021-84787-5#citeas.
3.
Instituto Nacional de câncer. Câncer: Como
surge o câncer? [Internet]. Rio de Janeiro: INCA;
2022. [citado 2022 Maio 06]. Disponível em: https://www.inca.gov.br/como-surge-o-cancer.
4.
Paiva EMC, Moraes CM, Brito TRP, Lima DB, Fava SMCL,
Nascimento MC. Perfil dos atendimentos oncológicos de uma macrorregião de saúde
brasileira. Avances en Enfermería [Internet]. 2020 [citado 2021 Jun 11];
38 (2): 149-58. Disponível em: https://revistas.unal.edu.co/index.php/avenferm/article/view/83297.
5.
Instituto
Nacional de câncer José Alencar Gomes da Silva. Estimativa 2020: incidência do
câncer no Brasil. Rio de Janeiro: INCA; 2019 [citado 2021 Jun 11]. Disponível
em: https://bit.ly/38MyYUb.
6.
Cavalcante JR, Santos ACC, Bremm JM, Lobo AP, Macário EM,
Oliveira WK, et al. COVID-19 no Brasil: evolução da epidemia até a semana
epidemiológica 20 de 2020. Epidemiol Serviços Saúde [Internet]. 2020 [citado
2021 Jun 11]; 29(4). Disponível em: https://doi.org/10.5123/S1679-49742020000400010.
7.
Coronavírus Brasil. Covid-19: Painel de controle. 2022
[citado 2022 Mar 14]. Disponível em: https://covid.saude.gov.br/.
8.
Doença do Doronavírus 2019 (COVID-19): Epidemiologia.
2021 [citado 2021 Jun 11]. Disponível em: https://bestpractice.bmj.com/topics/pt-br/3000201/epidemiology.
9.
Leite JS, Feter N, Caputo EL, Doring IR, Cassuriaga J,
Reichert FF, et al. Manejo de doenças crônicas não-transmissíveis durante a
pandemia de COVID-19: resultados da coorte PAMPA. Ciência Saúde Coletiva
[Internet]. 2021 [citado 2021 Jun 11]; 26(3): 987-1000. Disponível em:
https://doi.org/10.1590/1413-81232021263.39232020.
10.
Corrêa KM, Oliveira JDB, Taets GGCC. Impacto na Qualidade de
Vida de Pacientes com Câncer em meio à Pandemia de Covid-19: uma Reflexão a
partir da Teoria das Necessidades Humanas Básicas de Abraham Maslow. Rev
Bras Cancerol [Internet]. 2020 [citado 2021 Jun 11]; 66 (Tema Atual).
Disponível em:
https://www.semanticscholar.org/paper/Impacto-na-Qualidade-de-Vida-de-Pacientes-com-em-%C3%A0-Corr%C3%AAa-Oliveira/34a1387a299eb3b27997c651e0d2b4f74427569a.
11.
Rede
Câncer. Publicação trimestral do Instituto Nacional de Câncer José Alencar
Gomes da Silva. 46° Edition. 2020 [citado 2022 Jan 18]. Disponível em:
https://www.inca.gov.br/sites/ufu.sti.inca.local/files//media/document//redecancer-ed46-0610-web_-completo.pdf.
12.
Mendes
KDS, Silveira RCCP, Galvão CM. Use of the bibliographic reference manager in
the selection of primary studies in integrative reviews. Texto & Contexto –
Enfermagem [Internet]. 2019 [citado 2022 Jan 11]; 28. Disponível em:
https://doi.org/10.1590/1980-265X-TCE-2017-0204.
13.
Melnyk
BM, Fineout EO. Práticas baseadas em evidências em enfermagem e saúde: Um guia
para as melhores práticas. 4° ed. Philadelphia: Wolters Kluwer; 2019.
14.
Page MJ, Mckenzie JE, Bossuyt PM, Boutron I, Roffmann TC,
Mulrow CD, et al. A declaração PRISMA 2020: uma diretriz atualizada para
relatórios revisões sistemáticas. BMJ [Internet]. 2021 [citado 2022 Abr 18];
372(71). Disponível em: https://www.bmj.com/content/bmj/372/bmj.n71.full.pdf.
15.
Cavanna
L, Citterio C, Nunzio CD, Biasini C, Palladino MA, Ambroggi M, et al. Prevalence
of COVID-19 infecion in asymptomatic câncer patients in a district with high
prevalence of SARS-CoV-2 in Italy. Cureus [Internet]. 2021 [citado 2021 Dez
20]; 13(3): DOI: 10.7759/cureus.13774
16.
Elkin
E, Viele C, Schumacher K, Boberg M, Cunningham M, Liu L, et al. A covid-19
screening tool for oncology telefone triage. Suportive Care in Cancer
[Internet]. 2020 [citado 2021 Dez 20]; 29(4): DOI: 10.1007/s00520-020-05713-5.
17.
Ferrua
M, Mathivon D, Duflot-Boukobza A, Abbas M, Charles C, Barrais A, et al. Nurse
navigators’ letemonitoring for câncer patients with COVID-19: a French case
study. Support Care Cancer [Internet]. 2021 [citado 2021 dez. 20]; 29:
4485-4492. Disponível em: DOI: 10.1007/s00520-020-05968-y.
18.
Miashowski
C, Paul SM, Snowberg K, Abbott M, Borno H, Chang S, et al. Oncology patients’
perceptions of and experiences with COVID-19. Suportive Care in Cancer
[Internet]. 2021 [citado 2021 Dez 20]; 29: 1941-1859. Disponível em: DOI:
10.1007/s00520-020-05684-7.
19.
Pritchett
JC, Borah BJ, Desai AP, Xie Z, Saliba AN, Leventakos K, et al. Association
of a remote patient monitoring (RPM) program with reduced hospitalizations in
câncer patients with COVID-19. JCO Oncol Pract [Internet]. 2021 [citado 2021 Dez
20]; 17(9): 1293-302. Disponível em: DOI: 10.1200/OP.21.00307.
20.
Sampaio
SG dos SMS, Dias AM, Freitas R, Borsatto AZ, Esteves EMFL, de Oliveira LC.
Evalution of the criteria adopted to identify suspected cases of COVID-19 in
the emergency department service of a referral palliative oncology care unit.
American J Hospice palliative medicine [Internet]. 2021 [citado 2021 Dez 20];
38(2): 199-203. Disponível em: DOI: 10.1177/1049909120957310.
21.
Santiago
FB, da Silva ALA. Primeiro caso de COVID-19 em uma unidade de cuidados
paliativos oncológicos. Enferm. Foco [Internet]. 2020 [citado 2021 Dez 20];
11(2): 205-210. Disponível em: DOI: https://doi.org/10.21675/2357-707X.2020.v11.n2.ESP.3847.
22.
Strang
P, Hedman C, Aslitzer & Torbjorn S. Dying from cancer with COVID-19: age,
sex, socio-economic status, and comorbidities. Acta oncológica [Internet]. 2021
[citado 2021 Dez 20]; 60(8): 1019-1024. Disponível em: DOI:
10.1080/0284186X.2021.1934536.
23.
Silva
TC, Fortes RC, Ferrão PA. Percepção de pacientes oncológicos quanto ao
impacto da pandemia de COVID-19 frente ao diagnóstico e tratamento do câncer.
Braz J Development [Internet]. 2022 [citado 2022 Abr 18]; 8(1): 6508-6532.
Disponível em:
https://www.brazilianjournals.com/index.php/BRJD/article/view/43179/pdf.
24.
Vieira
MRS, Dias LRD, Andrade AFSM, Teles WS. Assistência à Pacientes
Oncológicos na era Covid-19: uma Revisão Integrativa. Braz J Health Review.
[Internet] 2021 [citado 2022 Abr. 18]; 4(3): 13990-14005. Disponível em:
DOI:10.34119/bjhrv4n3-335.
Scientific Editor: Ítalo Arão Pereira Ribeiro. Orcid: https://orcid.org/0000-0003-0778-1447
Rev Enferm Atual
In Derme 2023;97(2):e023098