ORIGINAL ARTICLE
DEVELOPMENT OF A CHECKLIST FOR THE PREVENTION OF PRESSURE INJURIES IN CRITICALLY ILL PATIENTS IN THE PRONE POSITION
ELABORACIÓN DE CHECKLIST PARA LA PREVENCIÓN DE LESIONES POR PRESIÓN EN EL PACIENTE CRÍTICO EN POSICIÓN PRONA
https://doi.org/10.31011/reaid-2026-v.100-n.1-art.2637
1Cléton Salbego
2Ana Caroline Bernardino Micelli
3Isabelle Gomes Facundin
4Jessika de Oliveira Cavalaro
5Robson Giovani Paes
6Liege Gonçalves Cassenote
1Docente do Curso de Graduação em Enfermagem do UniBrasil, Curitiba, Paraná, Brazil. ORCID: https://orcid.org/0000-0003-3734-9970
2Acadêmica do Curso de Graduação em Enfermagem do UniBrasil, Curitiba, Paraná, Brazil. ORCID: https://orcid.org/0009-0007-6234-2478
3Acadêmica do Curso de Graduação em Enfermagem do UniBrasil, Curitiba, Paraná, Brazil. ORCID: https://orcid.org/0009-0006-1878-3850
4Docente do Curso de Graduação em Enfermagem do UniBrasil, Curitiba, Paraná, Brazil. ORCID: https://orcid.org/0000-0002-4609-217X
5Programa de Pós-Graduação em Enfermagem da Universidade Federal do Paraná, Curitiba, Paraná, Brazil. ORCID: https://orcid.org/0000-0001-6899-4054
6 Programa de Pós-Graduação em Enfermagem da Universidade Federal de Santa Maria, Santa Maria, Rio Grande do Sul, Brazil. ORCID: https://orcid.org/0000-0003-0833-4016
Corresponding Author
Cléton Salbego
Rua Frei Egídio Carloto, 499, Curitiba/PR, Brazil. CEP: 81270-730 - +55 (55) 99922-1825, E-mail: cletonsalbego@hotmail.com
Submission: 30-08-2025
Approval: 28-02-2026
ABSTRACT
Objective: To develop a checklist for monitoring and preventing pressure injuries in patients in prone position admitted to adult intensive care. Method: This is a methodological study conducted between March and June 2025. A literature review was conducted in the following databases to develop the content and appearance of the checklist: Latin American and Caribbean Health Sciences Literature, Nursing Database, and Medical Literature Analysis and Retrieval System Online through the Virtual Health Library. Systematic reviews, recommendations/guidelines, and guidelines were consulted. Results: The literature search identified nine studies with recommendations for best practices for preventing pressure injuries in the prone position. Thus, the checklist was constructed containing three domains (Patient assessment and preparation; Care during prone positioning; Monitoring and reassessment). It was developed with the help of Microsoft Office Word software. Conclusion: The checklist presents relevant content to assist nursing professionals in preventing pressure injuries in critically ill patients undergoing prone positioning.
Keywords: Pressure Ulcer; Intensive Care Units; Critical Care Nursing; Checklist; Severe Acute Respiratory Syndrome.
RESUMO
Objetivo: Elaborar um checklist para o monitoramento e a prevenção de lesão por pressão no paciente em posicionamento prona, internado em terapia intensiva adulto. Método: Estudo metodológico, realizado entre março e junho de 2025. Para a construção do conteúdo e aparência do checklist foi realizada revisão da literatura nas bases de dados: Literatura Latino-Americana e do Caribe em Ciências da Saúde, Base de Dados de Enfermagem e Medical Literature Analysis and Retrievel System Online, por meio da Biblioteca Virtual em Saúde. Foram consultadas as revisões sistemáticas, recomendações/diretrizes e guidelines. Resultados: A busca na literatura permitiu identificar nove estudos com recomendações de boas práticas para prevenção de lesão por pressão em prona. O checklist contém 52 itens organizados em três domínios (avaliação e preparo do paciente; cuidados durante o posicionamento prona; monitoramento e reavaliação). Conclusão: O checklist apresenta conteúdo relevante para auxiliar profissionais de enfermagem na prevenção de lesões por pressão em pacientes críticos submetidos ao posicionamento prona.
Palavras-chave: Úlcera por Pressão; Unidades de Terapia Intensiva; Enfermagem de Cuidados Críticos; Lista de Checagem; Síndrome Respiratória Aguda Grave.
RESUMEN
Objetivo: Desarrollar una lista de verificación para el monitoreo y la prevención de lesiones por presión en pacientes en decúbito prono, ingresados en cuidados intensivos para adultos. Método: Estudio metodológico, realizado entre marzo y junio de 2025. Para elaborar el contenido y el aspecto de la lista de verificación, se revisó la bibliografía en las bases de datos: Literatura Latinoamericana y del Caribe en Ciencias de la Salud, Base de Datos de Enfermería y Medical Literature Analysis and Retrieval System Online, a través de la Biblioteca Virtual en Salud. Se consultaron las revisiones sistemáticas, recomendaciones/directrices y guías. Resultados: La búsqueda bibliográfica permitió identificar nueve estudios con recomendaciones de buenas prácticas para la prevención de lesiones por presión en decúbito prono. Por lo tanto, la lista de verificación se construyó conteniendo tres dominios (Evaluación y preparación del paciente; Cuidados durante el decúbito prono; Monitorización y reevaluación). Fue desarrollada con la ayuda del software Microsoft Office Word. Conclusión: La lista de verificación presenta contenido relevante para ayudar a los profesionales de enfermería en la prevención de lesiones por presión en pacientes críticos sometidos a decúbito prono.
Palabras clave: Úlcera por Presión; Unidades de Cuidados Intensivos; Enfermería de Cuidados Críticos; Lista de Verificación; Síndrome Respiratorio Agudo Grave.
INTRODUCTION
Severe Acute Respiratory Syndrome (SARS) is a clinical condition characterized by flu-like symptoms that can rapidly progress to respiratory failure, requiring hospitalization(1). SARS gained significant attention in health services during the Covid-19 pandemicdue to the high rate of associated complications and mortality. The clinical picture involves impaired gas exchange, worsening the condition of patients and requiring intensive medical attention(1).
Epidemiological surveillance of SARS in Brazil is systematically conducted by the Ministry of Health with the aim of monitoring the disease spread and guiding prevention and control measures. Significant variations in cases were observed between 2021 and 2024, with peaks during outbreaks of viral infections, such as Covid-19 and Influenza(2).
Critically ill patients with severe respiratory infections may develop Severe Acute Respiratory Syndrome (SARS). This condition is often associated with hypoxemic respiratory failure and has an unfavorable prognosis, especially when caused by viral infections(3). Given this, the therapeutic approach must be immediate and effective, aiming to reverse the clinical picture and reduce complications(3).
Protective ventilation becomes the protagonist in this scenario, guided by reduced tidal volumes and a positive expiratory pressure that respects alveolar time. Studies suggest that prone positioning is one of the few interventions which have demonstrated improvement in oxygenation and increased patient survival, and can be performed with awake or sedated patients, in different ventilatory support modes(3).
Prone positioning improves compatibility between ventilation and perfusion. Initially considered a rescue measure, this intervention has become standard therapy, with recommendations for sessions between 12 and 16 hours daily, although there is no definitive consensus on the ideal duration of use(4).
One of the risks associated with prolonged use of the prone position is pressure injuries (PI) caused by continuous pressure and shear forces on vulnerable tissues(5). Preventing such injuries involves a task that demands more than technique; it requires careful and critical observation in areas such as the face, chest, pelvis, knees, and feet. A systematic review with meta-analysis involving 15,979 patients in the prone position in the ICU identified an incidence of pressure injuries between 25.7% and 48.5%, highlighting the need for preventive measures. The results indicated the occurrence of injuries in 13 body regions, mainly in the face, chest, iliac crest, and knees(5). Another systematic review highlights checklists as a promising approach for applying evidence-based care(6), although their implementation in clinical practice faces challenges.
The interest in constructing the checklist was motivated by the authors’ care experience in the pandemic context regarding the high rates of PI resulting from the prone position. Given this, the need arises to strengthen the safety of critically ill patients and to support nurses in clinical decision-making. The nurse is the professional in adult ICU practice responsible for coordinating care, supervising the multidisciplinary team, and ensuring that preventive interventions are applied in a standardized manner. Therefore, the objective of this study was to develop a checklist for monitoring and preventing pressure injuries in patients in the prone position admitted to adult intensive care.
METHODS
This is a methodological study(7) conducted online between March and June 2025, with the objective of constructing the content (items and domains) and appearance (layout) for a pressure injury prevention checklist related to prone positioning of critically ill adult patients.
A literature review was conducted to construct the content of the checklist in the following databases: Latin American and Caribbean Literature in Health Sciences (LILACS), Nursing Database (BDENF) and Medical Literature Analysis and Retrieval System Online (MEDLINE), accessed through the Virtual Health Library (VHL). The searches took place in March, considering studies published between 2019 and 2024. A search strategy was developed using the controlled descriptors “coronavirus infections”, “prone position” and “pressure injury”, their synonyms and corresponding terms in English and Spanish. The strategy was organized by combining the descriptors with the Boolean operators AND and OR.
Systematic reviews, recommendations, clinical guidelines, and expert consensus in Portuguese, English, or Spanish were included. Duplicate documents with each being counted once in the database with the highest number of publications; documents which did not describe strategies for preventing pressure injuries in prone-positioned adult intensive care patients in their results; publications without scientific editing that were not indexed; and grey literature (theses, dissertations, course completion papers, handouts, proceedings, ordinances, and ministerial publications) were all excluded.
The studies were selected by independently reading the titles and abstracts by two authors in order to meet the inclusion criteria and identify nursing interventions for the prevention of pressure injuries in mechanically ventilated patients in the prone position, focusing on skin safety and integrity. A third reviewer was invited to analyze the study in case of doubt in the selection.
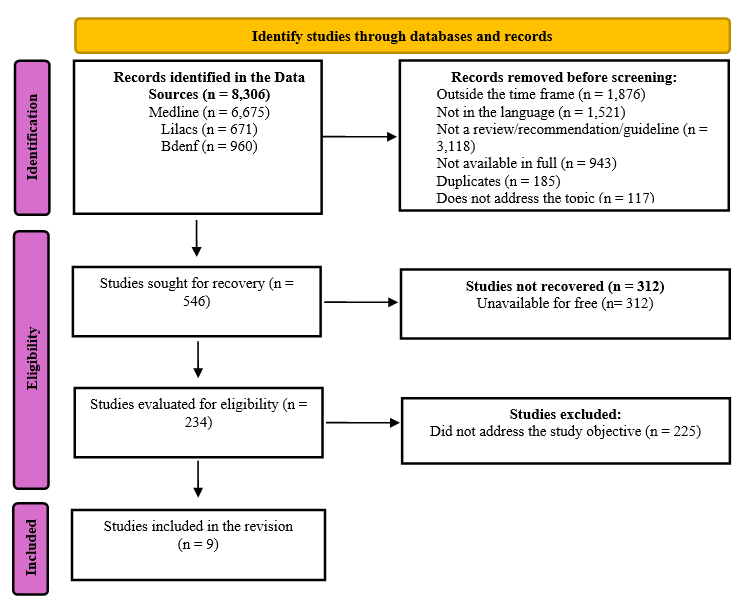
The selected evidence follows the classification proposed by the American Association of Critical-Care Nurses, which qualifies the results as: Level A - Meta-analysis of quantitative studies or meta-synthesis of qualitative studies with results that consistently support a specific action, intervention, or treatment (including systematic review of randomized clinical trials); Level B - Well-designed and controlled studies with results that consistently support a specific action, intervention, or treatment; Level C - Qualitative studies, descriptive or correlational studies, integrative reviews, systematic reviews, or randomized clinical trials with inconsistent results; Level D - Peer-reviewed professional and organizational standards, supported by recommendations from clinical studies; Level E - Multiple case reports, evidence based on theory of expert opinions, or peer-reviewed professional organizational standards, without clinical studies to support recommendations; Level M - Manufacturer recommendations only(8). A total of 8,306 documents were identified in the databases. After full reading, nine were selected for construction of the checklist (Figure 1).
Figure 1 - Flowchart representing the studies selected for construction of the checklist developed based on the PRISMA-ScR recommendation. Curitiba, PR, Brazil, 2025.
The selection of evidence considered systematic reviews and recommendations/guidelines, with emphasis on documents that presented summaries of good care practices applicable to the ICU context and prone position care. Technical Note No. 03/2017(9) from the National Health Surveillance Agency (Agência Nacional de Vigilância Sanitária - ANVISA) was consulted, which presents recommendations for safe practices for pressure injury prevention in Brazilian health services.
After data collection and organization, nursing interventions described in the selected documents were extracted, focusing on pressure injury prevention associated with prone positioning. The items were inductively developed by the researchers based on identification of recurrent, specific, and potentially measurable care actions, which were then grouped by semantic and functional similarity. The items were then organized into three thematic domains: (1) Patient assessment and preparation; (2) Care during prone positioning; and (3) Monitoring and reassessment.
In turn, six consensus meetings were held among the three authors of the study to ensure the content validity and internal consistency of the checklist, each lasting an average of one and a half hours, conducted via the Google Meet® platform. Decisions were made based on triangulation between scientific evidence, the researchers’ clinical experience, and adherence to the instrument’s scope. The discussions enabled evaluating the relevance, clarity, and applicability of the items, as well as a proposal of semantic and structural adjustments. This step constituted an internal content validation process based on consensus among the researchers(10).
The instrument was constructed using Microsoft Office Word® software, resulting in the first version of the checklist being composed of 52 items distributed across three domains: Domain 1 – Patient assessment and preparation (20 items); Domain 2 – Care during prone positioning (11 items); and Domain 3 – Monitoring and reassessment (21 items). The instrument was titled “Checklist for Pressure Injury Prevention in Critically Ill Adult Patients in the Prone Position”.
The analysis and organization of the checklist content were operationalized using the Content Analysis technique, following the methodological steps of pre-analysis, floating reading, coding, and thematic categorization. The corpus was composed of the scientific evidence obtained in the review, which was analyzed as units of meaning, meeting the criteria of exhaustiveness, representativeness, homogeneity, relevance, and exclusivity, as proposed by Bardin. Final interpretation of the data was guided by theoretical contributions from national and international literature focused on the prevention of pressure injuries and the safety of critically ill patients.
The recommendations of Strengthening the Reporting of Quality Improvement Studies in Health Care (SQUIRE 2.0)(11) were adopted to ensure scientific rigor and transparency in the methodological description of the study, being appropriate for this study design.
The research protocol was prepared in accordance with the ethical principles of Resolutions 466/2012 and 674/2022 of the National Health Council, and the guidelines of Circular Letter No. 2/2021. The project was approved by the Research Ethics Committee of the Autonomous University Center of Brazil, under opinion number 7.552.548 on May 7, 2025.
RESULTS
This review included nine studies for the construction of the checklist, which were classified according to the level of evidence (Table 1).
Table 1 - Characteristics of the studies selected for construction of the checklist for pressure injury prevention in critically ill adult patients in the prone position. Curitiba, PR, Brazil, 2025.
|
Authorship |
Title |
Journal / Year |
Level of evidence (AACN) |
|
|
1 |
Patton D. et al.(5) |
The effect of prone positioning on pressure injury incidence in adult ICU patients: A meta-review of systematic reviews |
Aust Crit Care. / 2022 |
A – Meta-review |
|
2 |
Lovegrove J, Fulbrook P, Miles S, Steele M.(6)
|
Effectiveness of interventions to prevent pressure injury in adults admitted to intensive care settings: A systematic review and meta-analysis of randomised controlled trials |
Aust Crit Care. / 2022 |
A – Meta-review |
|
3 |
Wang Z, et al.(12) |
Strategies to prevent pressure injuries among intensive care unit patients mechanically ventilated in prone position: a systematic review and a Delphi study |
Front Med (Lausanne) / 2023 |
A – Meta-review |
|
4 |
Pott F.S. et al.(13) |
Pressure injury prevention measures: overview of systematic reviews |
Rev Esc Enferm USP / 2023 |
A – Overview/ umbrella review |
|
5 |
Ibarra G. et al.(14) |
Prone position pressure sores in the COVID-19 pandemic: The Madrid experience |
J Plast Reconstr Aesthet Surg. / 2021 |
C – Observational study / narrative review |
|
6 |
EPUAP / NPIAP / PPPIA(15) |
Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline |
Diretriz internacional / 2019 |
D – Professional standards reviewed by peers, supported by clinical studies |
|
7 |
Agency for Clinical Innovation (NSW Health)(16) |
Preventing Pressure Injuries in Critically Ill Patients: Clinical Practice Guide |
Intensive Care NSW / 2024 |
D – Peer-reviewed organizational guideline, supported by clinical recommendations |
|
8 |
Team V, Jones A, Weller CD.(17) |
Prevention of Hospital-Acquired Pressure Injury in COVID-19 Patients in the Prone Position |
Intensive Crit Care Nurs. / 2022 |
C – Integrative review |
|
9 |
Morata L, Vollman K, Rechter J, Cox J.(18) |
Manual prone positioning in adults: Reducing the risk of harm through evidence-based practices (AACN Practice Alert) |
Crit Care Nurse. / 2024 |
E – Evidence based on expert consensus and professional practice |
Next, the evidence on the subject was examined with the aim of identifying which nursing interventions are necessary to compose the checklist aimed at preventing pressure injuries/ulcers in critically ill adult patients in the prone position (Table 2).
Table 2 - Synthesis of the best evidence on recommended practices for the prevention of pressure injuries/ulcers in critically ill adult patients in the prone position. Curitiba, PR, Brazil, 2025.
|
|
Recommendation |
Level of evidence |
|
1 |
Assess the skin and bones in areas with medical devices and when changing the patient’s position. |
C/D |
|
2 |
Place the patient on a pressure redistribution surface. |
C/D |
|
3 |
Perform small position changes at least every 2 hours while the patient is in the prone position and relieve vulnerable anatomical areas with positioning devices. |
D |
|
4 |
Apply prophylactic dressings to pressure points before prone positioning the patient (Forehead, maxilla, mandible, chin, clavicles, iliac crests, pubic symphysis, elbows, patellae, pretibial aspects, dorsum of the feet). |
B |
|
5 |
Remove prophylactic dressings if they become dislodged, soiled, or excessively wet. |
B |
|
6 |
Prevent and monitor skin injuries related to medical devices. Use a thin prophylactic dressing under medical devices, secure all tubes and devices away from the skin, empty ostomy bags, remove the urinary catheter fixation device from the thigh and place it toward the foot of the bed. |
D |
|
7 |
Protect and secure the airway with tape to minimize the risk of pressure injuries and ensure it is secure before turning the patient. |
D |
|
8 |
Designate someone to manage the airway at the head of the bed. Facilitate the presence of the provider in the area during the turning in case of accidental extubation. |
D/E |
|
9 |
Perform eye assessment daily before and after prone positioning. Clean the eyes with gauze moistened with saline solution and apply ointment. |
D |
|
10 |
Avoid direct pressure on the eyes. |
D |
|
11 |
Maintain straight spinal alignment and avoid excessive arm rotation and hyperextension of the neck. |
D |
|
12 |
Assess the patient for signs and symptoms of gastrointestinal intolerance (abdominal distension, regurgitation, vomiting). |
C |
|
13 |
Suspend the diet 1 hour before positioning the patient to allow gastric emptying. Resume feeding as soon as the patient is in the prone position. |
E |
|
14 |
Ensure ongoing education for the professionals involved. |
C/E |
|
15 |
Gather at least 5 trained professionals to perform the procedure. |
E |
|
16 |
Inflate the air mattress to the maximum to make the bed firm. |
E |
Source: elaborated by the authors, 2025.
In addition to pointing out the best practices to be adopted for preventing pressure injuries/ulcers in the prone position, the literature also indicates practices that are not recommended (Table 3).
Table 3 - Synthesis of evidence on non-recommended practices in the prevention of pressure injuries/ulcers in critically ill adult patients in the prone position. Curitiba, PR, Brazil, 2025.
|
|
Non-recommended practices |
Level of evidence |
|
1 |
Avoid the use of ring or donut-shaped support devices. |
D |
|
2 |
Shoulder extension positions. |
D |
|
3 |
Current guidelines do not recommend routine checking of gastric residual volumes (GRV) to assess GI intolerance. If GRV checks are an institutional standard, enteral nutrition should not be discontinued for GRV less than 500 mL in the absence of other signs of intolerance. |
D |
Source: elaborated by the authors, 2025.
The instrument entitled “Checklist for Pressure Injury Prevention in Critically Ill Adult Patients in the Prone Position” has 52 items, distributed across 3 domains: Domain 1 – Patient assessment and preparation (20 items); Domain 2 – Care during prone positioning (11 items); and Domain 3 – Monitoring and reassessment (21 items) (Table 4).
Table 4 - Checklist for pressure injury prevention in critically ill adult patients in the prone position. Curitiba, PR, Brazil, 2025.
|
Patient name: |
||||||
|
Date of Birth: |
Record: |
Bed: |
||||
|
Diagnosis: |
||||||
|
Date of Pronation: |
Time of Pronation: |
|||||
|
Date of Supination: |
Time of Supination: |
|||||
|
Legend: Y- Yes; N- No; NA- Not applicable |
|
|||||
|
Domains/Items |
Y |
N |
NA |
|
||
|
Domain 1. Patient assessment and preparation |
|
|
|
|
||
|
1. Perform hand hygiene according to aseptic technique. |
|
|
|
|
||
|
2. Adopt standard precaution measures. |
|
|
|
|
||
|
3. Adopt other precautionary measures, such as: ( ) Contact ( ) Aerosol ( ) Droplet. |
|
|
|
|
||
|
4. Suspend enteral feeding 1 (one) hour before prone positioning. |
|
|
|
|
||
|
5. Inflate the air mattress to its maximum capacity to make it firm. |
|
|
|
|
||
|
6. Identify signs of hyperemia and tissue involvement of the main bony prominences. ( ) forehead, ( ) maxilla, ( ) mandible, ( ) chin, ( ) clavicles, ( ) breasts, ( ) thorax, ( ) iliac crest, ( ) pubic symphysis, ( ) genitals, ( ) elbow, ( ) patella, ( ) tibia, ( ) dorsum of the foot, ( ) toes. |
|
|
|
|
||
|
7. Perform eye hygiene with 0.9% saline solution. |
|
|
|
|
||
|
8. Apply standardized eye ointment used at the institution. |
|
|
|
|
||
|
9. Secure the eyelids with adhesive tape. |
|
|
|
|
||
|
10. Assess the skin and bony prominences under and around medical devices. |
|
|
|
|
||
|
11. Protect with a thin prophylactic dressing and secure the endotracheal tube/tracheostomy cannula with adhesive tape or twill cotton tie. |
|
|
|
|
||
|
12. Check the positioning of the endotracheal tube, recording the measurement of the labial commissure. |
|
|
|
|
||
|
13. Empty the ostomy bag. |
|
|
|
|
||
|
14. Disconnect the urinary catheter from the vastus medialis region of the thigh, leaving it parallel to the body positioned at the foot of the bed. |
|
|
|
|
||
|
15. Apply prophylactic dressings to pressure points before prone positioning the patient. Note: hydrocolloid, thin foam, transparent film, or silicone dressings. |
|
|
|
|
||
|
16. Gather at least five professionals to perform the change from supine to prone position. |
|
|
|
|
||
|
17. Gather the necessary materials according to the institution’s availability and the patient’s physical constitution. |
|
|
|
|
||
|
18. Designate a physician to manage the airway at the head of the bed during the position change. |
|
|
|
|
||
|
19. Designate a leader to review the process and steps with the team before the turn and count to 3 before each movement to be performed. |
|
|
|
|
||
|
20. Instruct the professionals on the prone positioning procedure. |
|
|
|
|
||
|
Observations/Incidents:
|
|
|
|
|
||
|
Domain 2. Care during prone positioning |
|
|
|
|
||
|
21. Position the professionals appropriately. Note: 1 physician at the head of the bed, managing the airway; 2 professionals (nursing technician, nurse, or physiotherapist) on each side of the patient for chest and hip management. |
|
|
|
|
||
|
22. Check the need for the use of lifting assistance devices. Note: for patients weighing over 159 kg, or exceeding the minimum of 20 kg per professional. |
|
|
|
|
||
|
23. Use cushions and positioning aids to redistribute and relieve pressure on the head, trunk, elbows, and lower legs. Note: Avoid using ring or donut-shaped devices. |
|
|
|
|
||
|
24. Position the cushions on the chest and pelvis. |
|
|
|
|
||
|
25. Position the endotracheal tube in a way that allows for all movements. |
|
|
|
|
||
|
26. Check that all devices and tubes are securely positioned to prevent them from being pulled/tractioned or bent. |
|
|
|
|
||
|
27. Perform the ‘envelope’ technique in three steps: 1st - move the patient to the opposite side of the mechanical ventilation; 2nd - proceed with lateralization; 3rd - perform rotation to the prone position. |
|
|
|
|
||
|
28. Align the spine during and after the maneuver. |
|
|
|
|
||
|
29. Avoid excessive rotation of the arm. |
|
|
|
|
||
|
30. Elevate the head of the bed, placing the patient in a reverse Trendelenburg position of 15° to 25°. |
|
|
|
|
||
|
31. Support the head to avoid direct pressure on the patient’s eyes, preventing retinal damage. |
|
|
|
|
||
|
Observations/Incidents: |
||||||
|
Domain 3. Monitoring and reassessment |
|
|
|
|
||
|
32. Resume continuous 24-hour enteral nutrition as per provider instructions via the gastric route. |
|
|
|
|
||
|
33. Assess the patient for signs and symptoms of gastrointestinal intolerance. Examples: abdominal distension, regurgitation, vomiting. |
|
|
|
|
||
|
34. Recommend the use of prokinetic agents if symptoms of GI intolerance are present. |
|
|
|
|
||
|
35. Indicate placement of a post-pyloric tube for enteral nutrition if gastrointestinal intolerance is persistent. |
|
|
|
|
||
|
36. Assess skin and bony prominences when changing the patient’s position. Note: assess skin when changing arm position, facial areas when repositioning the head, and near medical devices. |
|
|
|
|
||
|
37. Perform micro-displacements and small position changes while the patient is prone to relieve vulnerable anatomical areas with positioning devices every 2 hours. |
|
|
|
|
||
|
38. Change the patient’s head position every 2 hours. |
|
|
|
|
||
|
39. Reposition the head every 4 hours based on the patient’s condition. |
|
|
|
|
||
|
40. Perform a daily ophthalmological evaluation to avoid direct pressure on the eyes and position the patient with the head of the bed elevated or in reverse Trendelenburg to reduce ocular edema and direct pressure on the head. |
|
|
|
|
||
|
41. Assess the skin under and around medical devices as part of the routine assessment during prone positioning and when returning the patient to the supine position. |
|
|
|
|
||
|
42. Maintain straight spinal alignment, avoiding excessive arm rotation as well as shoulder extension positions. |
|
|
|
|
||
|
43. Avoid positioning the arm in abduction beyond 70° with elbow extension and external shoulder rotation beyond 60°. |
|
|
|
|
||
|
44. Avoid hyperextension of the neck by adjusting the height of the head, chest, and pelvic supports. |
|
|
|
|
||
|
45. Assess specific pressure points during prone positioning, including face, chest, breasts, iliac crests, tibial plateau, pubic symphysis, genitalia, and toes and foot. |
|
|
|
|
||
|
46. Redistribute patient pressure using cushions, pillows, inflatable devices, fluidized positioners, and gel pads. Note: Use of donut or ring-shaped support devices should be avoided. |
|
|
|
|
||
|
47. Use a wedge with soft edges to elevate the patient’s feet so that their toes do not touch the surface. |
|
|
|
|
||
|
48. Assess prophylactic dressings, which should be removed if displaced, soiled, or excessively wet. |
|
|
|
|
||
|
49. Use liquid skin protectors or sealants on the face if there is excess moisture. Note: Consider using hydrofiber or calcium alginate for additional absorption. |
|
|
|
|
||
|
50. Keep tubes and devices away from the skin to prevent injury. |
|
|
|
|
||
|
51. Locate the endotracheal tube in an accessible manner. |
|
|
|
|
||
|
52. Monitor unit-specific pressure injury rates and incidences of airway displacement or obstruction, eye damage, brachial and ulnar injuries, gastrointestinal intolerance, and caregiver injuries related to patients positioned in the prone position. Note: This monitoring will help the team identify specific areas of practice that may require further assessment and remediation. |
|
|
|
|
||
|
Observations/Incidents: |
||||||
Source: elaborated by the authors, 2025.
DISCUSSION
The construction of a specific checklist for preventing pressure injuries (PI) during prone positioning represents a pragmatic strategy based on patient safety principles to systematize critical care involving multiple professionals and high technical complexity(1). Evidence described in meta-reviews and international guidelines shows although that prone positioning is a proven intervention to improve oxygenation in SARS, it is associated with a consistent increase in PI incidence due to pressure redistribution to previously less exposed surfaces (face, chest, pelvis, knees), which reinforces the need for specific and standardized preventive measures(5,6,19).
Structured instruments (checklists/bundles) emerge as adherence facilitators to evidence-based practices in the intensive care setting. Reviews on preventive interventions and studies which tested standardized protocols indicate that well-constructed checklists promote uniformity in actions, such as risk assessment, protection of bony prominences, eye care, secure fixation of devices, and frequent skin monitoring(19,20). These tools can reduce care variability which contributes to adverse events. Reviews on the use of bundles and protocols show a protective effect, although the certainty of the evidence varies according to the methodological heterogeneity of the studies evaluated(13).
Methodological studies in the Brazilian context have demonstrated the feasibility of constructing and validating care tools for patients in prone position or with pressure injuries/ulcers(21,22). A study validated the content and appearance of a checklist and banner on pressure injury/ulcer prevention in patients with Covid-19 in the prone position, showing acceptability among specialists and usefulness as an educational tool and support for clinical practice. These findings reinforce that in addition to the evidence stratified by the international literature, there is local scientific production focused on operationalizing prevention instruments(21).
In comparing other instruments for pressure injury/ulcer prevention in other positions (i.e. supine), it is observed that many principles are transversal: regular risk assessment, use of adequate support surfaces, protection of vulnerable areas, and frequent skin inspections; however, the prone position imposes additional requirements: systematic eye protection, airway management with permanent visibility of the endotracheal tube, and application of prophylactic dressings in anatomical locations not usually exposed, such as the face and chin(12). Thus, checklists for prone positioning need to include specific items (eye protection, lateral head rotation, facial prophylactic dressings, fixation and monitoring of the endotracheal tube), which may not be included or have less emphasis in protocols intended for the supine position. This differentiation is emphasized by studies which have mapped specific strategies for pressure injury/ulcer prevention in patients in the prone position(23,24).
Studies describe processes and instruments that are similar to the proposed checklist. The Standardized Pressure Injury Prevention Protocol (SPIPP) and standardized versions of pressure ulcer prevention checklists have shown validity and acceptability in hospital settings, serving as a model for adaptation to the ICU environment and the prone patient scenario; in addition, DNP projects and local initiatives (institutional protocols) report a reduction in adverse events after implementing prevention packages that include checklists, education, and continuous auditing(25). Furthermore, reviews indicate that the quality of evidence on the direct impact of isolated checklists on the incidence of pressure injuries/ulcers is heterogeneous. Studies combine multiple interventions (bundles, algorithms), which makes it difficult to isolate the effect of the checklist itself(12,20,22).
The literature also highlights critical components which should compose effective checklists for prone positioning: (1) pre-maneuver measures (hand hygiene, isolation precautions, suspension of enteral feeding when indicated, surface protection); (2) eye and face protection and surveillance; (3) fixation and verification of invasive devices with visible reference points; (4) use of prophylactic dressings appropriate to skin characteristics (foam, silicone, hydrocolloid); and (5) periodic skin monitoring and positioning microadjustments(12,13). All the items described are included in the checklist under analysis, and are supported by reviews on specific strategies for patients in the prone position.
Regarding effectiveness, studies that evaluated prevention packages show a reduction in injuries acquired in the hospital setting; however, the heterogeneity of design, small samples and frequent absence of randomized comparators limit the evidence consistency(13,20). For example, one overview concluded that combined interventions (bundles) tend to reduce hospital pressure injuries/ulcers, but the certainty of the evidence varies from low to moderate, reinforcing the need for controlled and multicenter studies focused on patients in the prone position to accurately quantify the impact of checklists/safeguards(13).
The limitations of this checklist reflect gaps evidenced in the literature: (a) a lack of unanimous consensus on which prophylactic dressing is superior for all anatomical situations in prone positioning; (b) variation in recommendations on optimal frequency of inspection and microrepositioning in hemodynamically unstable patients; and (c) a lack of randomized studies which isolated the effect of the checklist compared to usual care. Therefore, the need for content and appearance validation with experts and for usability assessment in the field is recognized(21,25).
This study contributes to clinical practice by offering a structured and evidence-based checklist that standardizes care during prone positioning, reduces variability in conduct, and strengthens the safety of the critically ill patient. The instrument facilitates early identification of risks, guides preventive interventions, and improves systematic monitoring of skin integrity, invasive devices, postural alignment, and eye protection.
In addition to improving the quality of care, the checklist promotes continuing education and multidisciplinary work, and can be incorporated into institutional protocols and quality improvement strategies. It also supports healthcare management by providing information for audits, decision-making, and cost reduction related to pressure injuries. Finally, the study fills gaps in the literature by proposing an applicable care technology, stimulating new validation and evaluation research, and expanding the scientific basis on preventing pressure injuries in the prone position.
FINAL CONSIDERATIONS
The pressure injury prevention checklist for critically ill adult patients in the prone position was constructed considering the best recommendations available in the international literature with a view to improving nursing care, promoting greater safety for patients with severe acute respiratory syndrome (SARS) susceptible to pressure injuries.
It is believed that the checklist will contribute to the care of critically ill adult patients in two ways: the first is related to nursing professionals, by providing a tool to aid decision-making; the second is linked to patient safety, as the instrument is characterized as a checklist with the potential to minimize adverse events resulting from care.
REFERENCES
1. Divisão de Vigilância Epidemiológica de Santa Catarina (DIVE-SC). Síndrome Respiratória Aguda Grave (SRAG) [Internet]. [citado 2025 Maio 18]. Disponível em: https://dive.sc.gov.br/index.php/sindrome-respiratoria-aguda-grave-srag.
2. Ministério da Saúde (BR). SRAG 2021 a 2024 - Banco de Dados de Síndrome Respiratória Aguda Grave - incluindo dados da COVID-19 [Internet]. Brasília-DF: Ministério da Saúde; 2024 [citado 2025 Maio19]. Disponível em: tthps://open15652cdatasus.saude.gov.br/dataset/srag-2021-a-2024/resource/8cb52f73-0184-41d5-8a8f-87d8f4
3. Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. 2020;8(5):475–481. Doi: https://doi.org/10.1016/s2213-2600(20)30079-5
4. Wang Y, Song J, Lin S, Zheng X, Zhao Z, Zhong M. Influence of prone position on regional ventilation/perfusion matching in patients with ARDS over time: a prospective physiological study. Respir Care. 2025 Mar 5;43(1):59-66. Doi: https://doi.org/10.1089/respcare.12247
5. Patton D, Latimer S, Avsar P, Walker RM, Moore Z, Gillespie BM, O'Connor T, Nugent L, Budri AMV, O'Brien NO, Chaboyer W. The effect of prone positioning on pressure injury incidence in adult intensive care unit patients: A meta-review of systematic reviews. Aust Crit Care. 2022;35(6):714-22. Doi: https://doi.org/10.1016/j.aucc.2021.10.003
6. Lovegrove J, Fulbrook P, Miles S, Steele M. Effectiveness of interventions to prevent pressure injury in adults admitted to intensive care settings: A systematic review and meta-analysis of randomised controlled trials. Aust Crit Care. 2022 Apr;35(2):186-203. Doi: https://doi.org/10.1016/j.aucc.2021.04.007
7. Lacerda MR, Costenaro RGS, organizadoras. Metodologias da pesquisa para Enfermagem e Saúde: da teoria à prática. 2ª ed. Porto Alegre: Moriá; 2018.
8. Peterson MH, Barnason S, Donnelly B, Hill K, Miley H, Riggs L, Whiteman K. Choosing the best evidence to guide clinical practice: application of AACN levels of evidence. Crit Care Nurse. 2014 Apr;34(2):58-68. Doi: https://doi.org/10.4037/ccn2014411
9. Ministério da Saúde (BR). Nota Técnica GVIMS-GGTES, n° 03 de 2017. Dispõe sobre as práticas seguras de prevenção de Lesão por Pressão em serviços de saúde. Brasília-DF: Anvisa; 2017. Disponível em: https://www.gov.br/anvisa/pt-br/centraisdeconteudo/publicacoes/servicosdesaude/notas-tecnicas/notas-tecnicas-vigentes/nota-tecnica-gvims-ggtes-no-03-2017.pdf/view
10. Salbego C, Nietsche EA. Praxis Model for Technology Development: a participatory approach. Rev Esc Enferm USP. 2023;57:e20230041. Doi: https://doi.org/10.1590/1980-220X-REEUSP-2023-0041en
11. Ogrinc G, Davies L, Goodman D, Batalden P, Davidoff F, Stevens D. SQUIRE 2.0 (Standards for QUality Improvement Reporting Excellence): revised publication guidelines from a detailed consensus process. Can J Diabetes. 2015;39(5):434-9. Doi: https://doi.org/10.1016/j.jcjd.2015.08.001
12. Wang Z, Fan J, Chen L, Xie L, Huang L, Ruan Y, Xu X, Liang Z. Strategies to preventing pressure injuries among intensive care unit patients mechanically ventilated in prone position: a systematic review and a Delphi study. Front Med (Lausanne). 2023 Aug 14;10:1131270. Doi: https://doi.org/10.3389/fmed.2023.1131270
13. Pott FS, Meier MJ, Stocco JGD, Petz FFC, Roehrs H, Ziegelmann PK. Pressure injury prevention measures: overview of systematic reviews. Rev Esc Enferm USP. 2023 Dec 22;57:e20230039. Doi: https://doi.org/10.1590/1980-220X-REEUSP-2023-0039en
14. Ibarra G, Rivera A, Fernandez-Ibarburu B, Lorca-García C, Garcia-Ruano A. Prone position pressure sores in the COVID-19 pandemic: The Madrid experience. J Plast Reconstr Aesthet Surg. 2021 Sep;74(9):2141-48. Doi: https://doi.org/10.1016/j.bjps.2020.12.057
15. European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel na Pan Pacific Pressure Injury Alliance. Prevenção e tratamento de lesões/úlceras por pressão. Guia de consulta rápida (Edição Portuguesa). Emily Haesler (Ed.). EPUAP/NPIAP/PPPIA: 2019.
16. Agency for Clinical Innovation (NSW Health). Preventing pressure injuries in critically ill patients: Clinical practice guide [Internet]. Chatswood (NSW): Agency for Clinical Innovation; 2020 [cited 2025 Nov 30]. Available from: https://aci.health.nsw.gov.au/__data/assets/pdf_file/0014/240152/ACI-Preventing-pressure-injuries-in-critically-ill-patients-clinical-practice-guide.pdf
17. Team V, Jones A, Weller CD. Prevention of Hospital-Acquired Pressure Injury in COVID-19 Patients in the Prone Position. Intensive Crit Care Nurs. 2022 Feb;68:103142. Doi: https://doi.org/10.1016/j.iccn.2021.103142
18. Morata L, Vollman K, Rechter J, Cox J. Manual Prone Positioning in Adults: Reducing the Risk of Harm Through Evidence-Based Practices. Crit Care Nurse. 2024 Feb 1;44(1):e1-e9. Doi: https://doi.org/10.4037/ccn2023201
19. Schaller SJ, Scheffenbichler FT, Bein T, et al. Diretriz sobre posicionamento e mobilização precoce em pacientes críticos elaborada por um painel de especialistas. Intensive Care Med. 2024;50:1211–27. Doi: https://doi.org/10.1007/s00134-024-07532-2
20. Chaboyer W, Latimer S, Priyadarshani U, Harbeck EL, et al. The effect of pressure injury prevention care bundles on pressure injuries in hospital patients: a complex intervention systematic review and meta-analysis. Int J Nurs Stud. 2024;155:104768. Doi: https://doi.org/10.1016/j.ijnurstu.2024.104768
21. Santos VB, Aprile DCB, Lopes CT, Lopes JL, Gamba MA, Costa KAL, et al. COVID-19 patients in prone position: validation of instructional materials for pressure injury prevention. Rev Bras Enferm. 2021;74(Suppl 1):e20201185. Doi: http://dx.doi.org/10.1590/0034-7167-2020-1185
22. Pinheiro RV, Salomé GM, Miranda FD, Alves JR, Reis FA, Mendonça ARA. Algoritmos para prevenção e tratamento de lesões por fricção. Acta Paul Enferm. 2021;34:eAPE03012. Doi: http://dx.doi.org/10.37689/acta-ape/2021AO03012
23. Gefen A, Brienza DM, Cuddigan J, Haesler E, Kottner J. Our contemporary understanding of the aetiology of pressure ulcers/pressure injuries. Int Wound J. 2022;19(3):692–704. Doi: https://doi.org/10.1111/iwj.13736
24. Wiegand DL, Carlson K, Richards K, et al. Team-based approach to prone positioning in COVID-19 patients: A step-by-step guide. Crit Care Nurse. 2021;41(1):16–27. Doi: https://doi.org/10.4037/ccn2021992
25. Özkan ÇG, Kurt Y, Öztürk H. Standardised Pressure Injury Prevention Protocol (SPIPP-Adult) Checklist 2.0: language and content validity study. J Eval Clin Pract. 2025;31:e14285. Doi: https://doi.org/10.1111/jep.14285
Funding and Acknowledgments:
Nothing to declare.
Data Availability Statement
No databases were generated in this study. The information presented is described in the body of the article.
Authorship Criteria (Authors' Contributions)
Ana Caroline Bernardino Micelli; Isabelle Gomes Facundin; Cléton Salbego - 1. Contributed substantially to the conception and/or planning of the study; 2. To the obtaining, analysis and/or interpretation of the data; 3. As well as to the writing and/or critical review and final approval of the published version.
Jessika de Oliveira Cavalaro; Robson Giovani Paes; Liege Gonçalves Cassenote - 3. Contributed to the writing and/or critical review and final approval of the published version.
Conflict of Interest Statement
Nothing to declare
Scientific Editor: Ítalo Arão Pereira Ribeiro. Orcid: https://orcid.org/0000-0003-0778-1447
Rev Enferm Atual In Derme 2026;100(1): e026030
![]()