REVIEW ARTICLE
NURSING CARE FOR PREVENTING PRESSURE INJURIES IN INTENSIVE CARE UNITS: AN INTEGRATIVE LITERATURE REVIEW
CUIDADOS DE ENFERMAGEM NA PREVENÇÃO DE LESÕES POR PRESSÃO EM UNIDADES DE TERAPIA INTENSIVA: REVISÃO INTEGRATIVA DA LITERATURA
CUIDADOS DE ENFERMERÍA PARA LA PREVENCIÓN DE LESIONES POR PRESIÓN EN UNIDADES DE CUIDADOS INTENSIVOS: UNA REVISIÓN INTEGRADORA DE LA LITERATURA
https://doi.org/10.31011/reaid-2026-v.100-n.1-art.2677
1José Macedo de Almeida
2Belarmino Santos de Sousa Júnior
3Bárbara Maria Lopes da Silva Brandão
4Karyne Kirley Negromonte Gonçalves
5Thaíse Alves Bezerra
1Graduando em Enfermagem. Faculdade Integrada CETE – FIC. Garanhuns – Pernambuco, Brazil. ORCID: https://orcid.org/0009-0008-7372-0902
2Doutor em Enfermagem. Programa de Pós-Graduação em Enfermagem da Universidade Federal de Pernambuco (PPGENF/UFPE). Faculdade Integrada – CETE – FIC, Garanhuns – Pernambuco, Brazil. ORCID: https://orcid.org/0000-0003-1780-1878
3Mestre em Enfermagem. Universidade Federal da Paraíba (UFPB). Faculdade Integrada – CETE – FIC, Garanhuns – Pernambuco, Brazil. ORCID: https://orcid.org/0000-0002-6652-9615
4Doutora em Enfermagem pelo Programa de Pós-Graduação em Enfermagem pela Universidade Federal de Pernambuco - UFPE. Universidade Federal de Pernambuco, Recife – Pernambuco, Brazil. ORCID: https://orcid.org/0000-0002-0205-4112
5Doutora em Enfermagem pelo Programa de Pós-Graduação em Enfermagem da Universidade Federal da Paraíba. Universidade Federal da Bahia - UFBA. Salvador – Bahia, Brazil. ORCID: https://orcid.org/0000-0003-3242-4468
Corresponding Author
José Macedo de Almeida
Rua Moisés Ferreira Calado, nº 24, Capoeiras-PE, Brazil, CEP 55365-000. phone: +55 (87)99126-3744. E-mail: jos3cpmacedo17@gmail.com.
Submission: 22-10-2025
Approval: 02-03-2026
ABSTRACT
Objective: To describe nursing care for preventing pressure injuries in intensive care units. Methods: This is an integrative literature review, conducted by cross-referencing standardized descriptors using the Health Sciences Descriptors/Medical Subject Headings in scientific databases such as the Scientific Electronic Library Online, Cumulative Index to Nursing and Allied Health Literature, and the Cochrane Library. The review was conducted between November 2024 and March 2025. Results: The application of scales, such as Braden and the Escala de Valoración Actual del Riesgo de desarrollar Úlceras por presión en Cuidados Intensivos (EVARUCI), frequent repositioning, skin hydration, the use of support surfaces and training of the nursing team were highlighted as essential nursing care for injury prevention. Conclusion: Nursing is essential for preventing pressure injuries, highlighting the importance of continuing education, constant monitoring, and the implementation of institutional protocols to ensure safe and effective care.
Keywords: Pressure Injury; Intensive Care; Nursing Care; Risk Factors; Clinical Protocols.
RESUMO
Objetivo: descrever os cuidados de enfermagem na prevenção de lesões por pressão em unidades de terapia intensiva. Métodos: trata-se de uma revisão integrativa da literatura, realizada por meio do cruzamento dos Descritores em Ciências da Saúde/Medical Subject Headings, nas bases de dados científicos como Scientific Electronic Library Online, Cumulative Index to Nursing and Allied Health Literature, Cochrane Library, realizada entre novembro de 2024 e março de 2025. Resultados: A aplicação das escalas, como de Braden e a Escala de Valoración Actual del Riesgo de desarrollar Úlceras por presión en Cuidados Intensivos (EVARUCI), o reposicionamento frequente, a hidratação da pele, o uso de superfícies de suporte e o treinamento da equipe de enfermagem foram evidenciados como cuidados de enfermagem essenciais para a prevenção de lesões. Conclusão: a atuação da enfermagem é fundamental na prevenção de lesões por pressão, destacando-se a importância da educação permanente, do monitoramento constante e da implementação de protocolos institucionais para garantir uma assistência segura e eficaz.
Palavras-chave: Lesão por Pressão; Terapia Intensiva; Cuidados de Enfermagem; Fatores de Risco; Protocolos Clínicos.
RESUMEN
Objetivo: Describir los cuidados de enfermería para la prevención de lesiones por presión en unidades de cuidados intensivos. Métodos: Se trata de una revisión integradora de la literatura, realizada mediante el cruce de descriptores estandarizados utilizando los Descriptores en Ciencias de la Salud/Encabezados de Temas Médicos, en bases de datos científicas como Scientific Electronic Library Online, Cumulative Index to Nursing and Allied Health Literature y Cochrane Library. La revisión se realizó entre noviembre de 2024 y marzo de 2025. Resultados: Se destacaron como cuidados de enfermería esenciales para la prevención de lesiones la aplicación de escalas, como la Braden y la Escala de Valoración Actual del Riesgo de desarrollar Úlceras por presión en Cuidados Intensivos (EVARUCI), el reposicionamiento frecuente, la hidratación de la piel, el uso de superficies de apoyo y la capacitación del equipo de enfermería. Conclusión: La enfermería es esencial para la prevención de lesiones por presión, destacando la importancia de la educación continua, el monitoreo constante y la implementación de protocolos institucionales para garantizar una atención segura y efectiva.
Palabras clave: Lesión por Presión; Cuidados Intensivos; Atención de Enfermería; Factores de Riesgo; Protocolos Clínicos.
INTRODUCTION
The hospital environment, while primarily intended for patient care and recovery, is also susceptible to various risks that can compromise the safety of everyone involved. Among these risks, Healthcare-Associated Infections (HAIs) stand out, frequently associated with contact with contaminated surfaces and invasive procedures. These infections can progress to serious conditions, such as sepsis, significantly increasing mortality and hospital costs 1.
In Intensive Care Units (ICUs), critically ill patients are particularly vulnerable to infections, especially when they have skin lesions. These conditions can progress to sepsis, characterized by a systemic inflammatory response that can lead to septic shock, culminating in multiple organ failure and, eventually, death. Thus, infectious complications in the ICU contribute significantly to increased mortality rates 2.
Among the most prevalent risks in this environment, pressure injuries (PIs) stand out, affecting mainly immobilized or sedated patients, representing one of the main threats to the quality of hospital care. Its higher incidence in ICUs is related to the inability of these patients to move, which increases their susceptibility to developing these injuries3.
According to the National Pressure Injury Advisory Panel (NPIAP), PIs are defined as localized damage to the skin and/or underlying tissues, usually over a bony prominence, resulting from prolonged pressure, with or without friction and shear 4. Its etiology involves intrinsic factors such as reduced mobility, nutritional status, age, chronic diseases, and hydration, and extrinsic factors such as prolonged pressure, friction, shear, moisture, and the use of medical devices. Knowledge of these factors is essential to understand the causes and plan effective prevention strategies 5.
Internationally, reviews and meta-analyses show that the burden of pressure ulcers remains substantial: pooled studies indicate a prevalence of 10 to 16%, with hospital incidence in the ICU depending on the region and study design. Regions and samples vary; for example, a global meta-analysis found that 1 in 10 hospitalized patients are affected; another ICU-focused review reported a prevalence of around 16% in some regions. Brazilian figures (12.7 to 14.9%) are within the same range as international estimates for ICU in various regions, i.e., they are not atypical, but confirm that pressure ulcers are a relevant problem in critical care 6-7.
Between 2014 and 2021, more than 100,000 cases of Adverse Events (AEs) related to pressure ulcers were reported in Brazilian hospitals, with emphasis on the most severe stages: stage 3 (14,808 cases, with exposure of adipose tissue) and stage 4 (4,670 cases, with exposure of bones and muscles). Studies indicate that, although most pressure ulcers occur in early stages, the deep stages (3 and 4), despite being less frequent, are those that demand greater resource consumption, significantly prolong hospitalization time, and generate a greater economic impact on health systems. Economic reviews highlight that most of the total cost comes precisely from these deep stages. These numbers show that pressure ulcers are among the main categories of adverse events, especially in critically ill patients6-7.
The National Patient Safety Program (PNSP), established in 2013 in Brazil, sets as one of its goals the prevention and control of pressure ulcer progression. The program emphasizes that these lesions prolong hospitalization time, increase hospital costs, and cause physical, mental, and emotional repercussions, especially for bedridden patients and those with reduced mobility due to the severity of their clinical condition 8.
Considered a preventable adverse event, pressure ulcers are directly related to the quality of care provided. Their prevention is the responsibility of the entire multidisciplinary team; however, the role of nursing is central, given its continuous involvement in the care process. Among the main preventive measures are the systematic assessment of skin integrity, frequent repositioning or changes of position, and the use of appropriate support surfaces 9.
Evidence demonstrates that nursing care is crucial in the prevention and management of pressure ulcers. The implementation of evidence-based practices allows for the early identification of signs of these lesions, favoring effective interventions at a critical moment during hospitalization. Thus, the nurse acts as a fundamental agent in reducing risks and promoting patient well-being, consolidating themselves as a guardian of quality of life in the intensive care unit 10-11.
Given the above and considering the relevance of nursing care, this study aims to describe nursing care in the prevention of pressure ulcers in intensive care units.
METHODS
This is an integrative literature review, whose objective was to explore and synthesize the available evidence regarding nursing care in the prevention of pressure ulcers in patients admitted to the ICU. This type of review allows for a broad analysis of the topic, enabling not only the gathering of existing knowledge but also the identification of gaps in clinical practice 12.
The study was guided by the Population–Concept–Context (PCC) strategy, as described in Chart1, which allowed for the structured definition of the research question and search criteria.
Chart 1 - Application of the PCC strategy. Garanhuns, Pernambuco, Brazil, 2025.
|
Acronym |
Definition |
Application |
|
P |
Population (População) |
Hospitalized Patients. |
|
C |
Concept (Conceito) |
Prevention of Pressure Injuries. |
|
C |
Context (Contexto) |
Nursing care practices in Intensive Care Units. |
Source: Authors' own work, 2025.
Based on the application of the PCC acronym, the following guiding question was formulated: "What nursing care measures can be implemented in Intensive Care Units to ensure that the risk of developing pressure injuries is minimized?". This formulation guided the entire process of searching, selecting, and analyzing the studies included in this review.
This study also adopted the Feasible, Interesting, Novel, Ethical, Relevant (FINER) criteria, used to assess the feasibility and relevance of research. The application of this strategy contributed to ensuring a guiding question that was feasible, interesting, innovative, ethically appropriate, and relevant to clinical practice and the advancement of scientific knowledge (Chart 2).
Chart 2 - Application of FINER criteria. Garanhuns, Pernambuco, Brazil, 2025.
|
Criterion |
Definition |
Application to the study |
|
F – Feasible (Viável) |
The research must be feasible in terms of time, resources, and access to information. |
Conducting an integrative review is feasible considering the availability of scientific databases and up-to-date literature on pressure injury prevention in the ICU. |
|
I – Interesting (Interessante) |
The topic should spark interest among researchers and the scientific community. |
Nursing care in the prevention of pressure ulcers in critically ill patients is of great relevance to professionals, managers, and researchers in the health field. |
|
N – Novel (Inovador) |
The research should add new information or confirm relevant data. |
This study gathers and synthesizes recent evidence, updating preventive practices according to current protocols and national/international guidelines. |
|
E – Ethical (Ético) |
Research must respect ethical principles. |
Since this is a literature review, there is no direct involvement of human beings, eliminating risks and maintaining compliance with ethical principles. |
|
R – Relevant (Relevante) |
Research should contribute to the advancement of knowledge and improvements in practice. |
The study provides insights to improve nursing care and reduce the incidence of pressure ulcers in the ICU, promoting patient safety. |
Source: Authors' own work, 2025.
Data collection took place between November 2024 and March 2025, encompassing the stages of searching, screening, eligibility, and analysis of the included studies. The search strategy was applied to the databases Scientific Electronic Library Online (SciELO), Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Cochrane Library.
Study selection was performed independently by two reviewers through reading titles and abstracts, followed by analysis of the full text of potentially eligible articles. Disagreements were resolved by consensus and, when necessary, through arbitration by a third reviewer.
The Mendeley® software was used for reference management and bibliographic organization. The identification and removal of duplicate studies, as well as the blind screening process of articles, were conducted on the Rayyan® platform.
To ensure a comprehensive and accurate search, Health Sciences Descriptors/Medical Subject Headings (DeCS/MeSH) and their combinations with Boolean operators were used. The search strategy performed in the SciELO database was executed using the following terms: ("Pressure Injury" OR "Pressure Ulcer") AND ("Nursing Care" OR "Nursing Assistance") AND "Prevention" AND ("Critical Care" OR "Intensive Care Unit"). The search in the CINAHL database used the following DeCS/MeSH terms: ("Primary Health Care" OR "Family Health Strategy") AND (nurse role) AND (patient satisfaction) AND ("Pressure Injuries" OR "Pressure Ulcer") AND (prevention protocol) AND (Intensive Care Units). The following DeCS/MeSH terms were used in the Cochrane Library database search: ("Intensive Care Units" OR ICU OR "Critical Care") AND ("Pressure Ulcer Prevention" OR "Pressure Injury Prevention" OR "Support Surfaces" OR Repositioning OR "Prophylactic Dressings" OR "Nursing Care") AND ("Pressure Ulcer" OR "Pressure Injuries").
Articles available in full and free of charge in the selected databases, published between 2013 and 2025, in Portuguese, English, or Spanish, addressing the topic, were included, encompassing qualitative, quantitative, mixed studies and literature reviews, empirical research, clinical trials, systematic reviews, and evidence-based guidelines.
Studies that did not directly address pressure injury prevention, studies restricted to treatment, studies targeting only pediatric or obstetric patients, studies that did not specify the role of nursing, or studies that were duplicated in the searched databases were excluded. To ensure that the results of this integrative review were based on solid evidence directly related to the central theme, exclusion criteria were established, disregarding opinion articles, editorials, conference abstracts, studies that did not directly address pressure injury prevention strategies, publications unavailable in full, and duplicated works in different databases.
The selection of articles followed specific eligibility criteria, considering publications between 2013 and 2025, a period that encompasses the establishment of the National Patient Safety Program (PNSP) and the dissemination of the new guidelines from the National Pressure Injury Advisory Panel (NPIAP) for pressure injury prevention. Initially, duplicate articles were removed, and then screening was carried out through title and abstract analysis. The shortlisted articles underwent full-text reading to assess their relevance and methodological quality. For the analysis of the included studies, data regarding the year of publication, methodological design, objectives, main results, and conclusions were extracted, allowing for the synthesis and comparison of findings. Only studies that fully met the inclusion criteria were analyzed in depth and incorporated into the review.
To classify the level of evidence of the analyzed studies, the hierarchy proposed by the Oxford Centre for Evidence-Based Medicine was adopted, which organizes research types according to their scientific robustness. At the top of the pyramid (level 1) are systematic reviews of randomized clinical trials and randomized trials themselves with high precision in their results. Level 2 includes systematic reviews of cohort studies and well-conducted cohort studies, as well as randomized trials with methodological limitations. Level 3 encompasses systematic reviews and case-control studies, while level 4 includes case series and observational studies with less methodological rigor. Finally, level 5 corresponds to expert opinions and reports not based on empirical evidence 13.
This rigorous selection process ensured the consistency and reliability of the data presented. The methodological flow was conducted according to the steps recommended by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), including the phases of identification, screening, and inclusion of studies, as illustrated in Figure 1 14.
Figure 1 - Presentation of Selected Articles. Garanhuns, Pernambuco, Brazil, 2025.
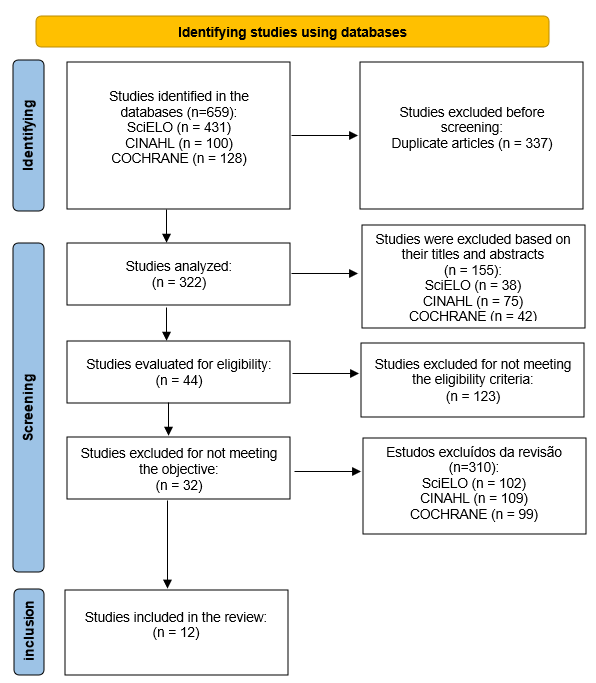
Source: Authors' own work, 2025.
RESULTS
The results are presented in a single table. This table contains specific information for each article in the sample, such as author(s), study location and year of publication, method, main results related to pressure injury prevention care, and level of evidence (Chart 3).
Chart 3 - Characterization of articles according to title, author, location and year of publication, method, results and level of evidence. Garanhuns, Pernambuco, Brazil, 2025.
|
ID* |
Article Title |
Country - Year |
Methods |
Key Results for Pressure Injury Prevention |
NE** |
|
1 |
Prevenção de lesão por pressão no contexto hospitalar: uma revisão sistemática 16 |
Brazil 2020 |
Systematic Review |
The review highlighted the use of different support surfaces (foam, gel, and alternating air) as essential resources in the prevention of pressure ulcers, as well as the use of photographs for greater diagnostic accuracy. Furthermore, it emphasized staff training and frequent changes in patient position as indispensable complementary measures. |
1 |
|
2 |
Comparing the Braden and Jackson/Cubbin pressure injury risk scales in trauma-surgery ICU patients 17 |
United States 2020 |
Retrospective Study |
The Jackson and Cubbin Scales demonstrated superior predictive and discriminatory properties compared to the Braden Scale for predicting pressure injury risk in critically ill trauma-surgical patients. |
2 |
|
3 |
Pressure injury prevention practice in Australian intensive care units: a national cross-sectional survey 18 |
Australia 2021 |
Clinical Trial |
Pressure ulcer prevention strategies in ICUs involved early risk assessment, structured repositioning, use of skin barriers, prophylactic dressings, and clinical audits. On a smaller scale, preventive rounds, safety meetings, and research on the topic were highlighted. It was also observed that skin integrity services were more frequent in metropolitan ICUs, while the involvement of occupational therapists occurred mainly in regional units. |
1 |
|
4 |
Relação entre o diagnóstico risco de lesão por pressão e a escala de Braden 19 |
Brazil 2021 |
Cross-sectional study |
Among the main prevention strategies observed in the study, the following stand out: systematic application of the Braden scale, prescription of personalized care, such as repositioning, skin care, use of mattresses or pressure-relieving surfaces, and monitoring for early signs of injury. |
2 |
|
5 |
Prevention of endotracheal tube-related pressure injury: a systematic review and meta-analysis 20 |
United States 2022 |
Systematic Review with Meta-analysis |
Interventions to reduce pressure ulcers related to tracheostomy included adjustments to fixation with foam collars, use of extended tubes, and application of hydrophilic dressings, the latter with proven benefit by meta-analysis. However, limited standardization of practices was observed among the studies. |
1 |
|
6 |
Improving pressure injury prevention by using wearable sensors to cue critical care patient repositioning 21 |
Untied States 2022 |
Clinical trial |
The study showed that adherence to repositioning increased from 55% to 89%, with a reduction in the interval between position changes. Furthermore, it highlighted improvements in nursing teamwork and a positive impact on pressure ulcer prevention. |
1 |
|
7 |
Implementation and evaluation of multilayered pressure injury prevention strategies in an Australian intensive care unit setting 22 |
Canada 2022 |
Clinical trial |
During the study, 15.4% of patients developed pressure ulcers, most of which were related to medical devices (73.2%). After adopting preventive strategies targeting both staff and patients, there was a significant reduction in rates, with a decrease of more than 50% in the risk of pressure ulcers. |
1 |
|
8 |
Assistência de enfermagem e fatores de risco na prevenção de lesão por pressão 23 |
Brazil 2023 |
Study of Review Integrative |
The authors highlight the importance of early recognition of risk factors. Among the most cited actions are: frequent skin assessment, the use of scales such as the Braden scale, regular patient mobilization, and systematic recording of care provided, and they emphasized the importance of unit control (microclimate). |
4 |
|
9 |
Instrumentos preditores de risco para lesão por pressão em pacientes críticos 24 |
Brazil 2024 |
Observational, Analytical, and Prospective Study |
The study indicated that the Escala de Valoración Actual del Riesgo de desarrollar Úlceras por presión en Cuidados Intensivos (EVARUCI) proved to be more sensitive and better adapted to the reality of the Intensive Care Unit compared to the Braden scale. |
3 |
|
10 |
Prevenção de lesão por pressão em unidade de terapia intensiva: implementação de melhores práticas25 |
Brazil 2024 |
Quasi-experimental study l |
The study highlighted the following as the main strategies for preventing pressure injuries: systematic risk assessment using the Braden scale, repositioning every two hours, use of alternating pressure mattresses, daily skin inspection, application of protective barriers in vulnerable areas, and the adoption of institutional protocols and clinical audits to reinforce adherence to best practices. |
3 |
|
11 |
Incidência de lesão por pressão em pacientes críticos com e sem COVID-19: estudo de coorte 26 |
Brazil 2024 |
Cohort Study |
Among the main strategies used to prevent injuries, the following stood out: application of the Braden scale for risk assessment, frequent repositioning of patients, care with skin hydration, use of specialized support surfaces, and involvement of the multidisciplinary team in the daily monitoring of skin conditions. |
3 |
|
12 |
Incidence of pressure injury in patients with moderate and severe traumatic brain injury: a systematic review 27 |
UK 2024 |
Systematic Review |
Pressure ulcer prevention strategies involved the judicious use of risk scales, such as the Braden scale and instruments adapted for neurological patients, combined with frequent changes in position, skin care, and the use of high-tech support surfaces. |
1 |
Source: Authors' own work, 2025.
*ID= Article Identification; **NE= Level of Evidence.
The review identified a wide variety of technologies and resources aimed at preventing pressure ulcers in intensive care units. Among them, specialized support surfaces, such as foam, gel, and alternating air mattresses, stood out, as well as the use of photographs as an auxiliary tool to increase the accuracy and reliability in the classification of injuries 16.
In addition, continuous training of the nursing staff and frequent changes in position proved to be indispensable complementary measures for safe care. Specific interventions, such as modifications in tracheostomy fixation and the use of hydrophilic dressings under the flanges, were also associated with a reduction in pressure ulcers related to medical devices, although the standardization of these practices is still limited 16,18-21,25-27.
Regarding predictive scales, instruments such as the Jackson and Cubbin Scale, as well as the EVARUCI, demonstrated greater sensitivity and discriminative capacity compared to the Braden scale, especially in the context of critically ill, neurological, and trauma-surgical patients. Even so, the Braden scale remained the most widely used tool, particularly when associated with institutional protocols, individualized care, and systematic records of skin assessment and pressure ulcer risk 17,19,23-27.
Prevention strategies involved early risk assessment upon admission, structured and frequent repositioning, use of skin barriers and prophylactic dressings in vulnerable areas, as well as clinical audits, safety rounds, and quality improvement projects. The results showed that the adoption of repositioning protocols increased team adherence from 55% to 89%, with average intervals of two to three hours, positively impacting teamwork and reducing pressure ulcer rates 21. Globally, 15.4% of patients developed pressure ulcers during the evaluated period, most of which were related to medical devices; however, after the implementation of structured strategies, there was a significant reduction in these rates (OR = 0.41; p = 0.0126) 22.
The synthesis of the analyzed evidence demonstrates that early recognition of risk factors, adequate microclimate control, and integrated action by the multidisciplinary team are key elements in improving care and reducing the incidence of pressure injuries in critically ill patients23.
DISCUSSION
The discussion was structured around thematic axes, in order to favor clarity of analysis and understanding of the results in light of the scientific literature. This approach allowed the evidence to be organized into categories related to available technologies, team training, risk prediction scales, institutional strategies, impacts on clinical practice, and key elements for the effective prevention of pressure injuries.
Available Technologies and Resources
The results of this review reinforce the importance of support technologies in the prevention of pressure injuries in Intensive Care Units. The use of special surfaces, such as high-density foam, gel, and alternating air mattresses, was frequently cited by studies as a priority intervention for reducing pressure on bony prominences. These results are in line with international recommendations from the National Pressure Injury Advisory Panel (NPIAP), the European Pressure Ulcer Advisory Panel (EPUAP), and the Pan Pacific Pressure Injury Alliance (PPPIA), which indicate such surfaces as a first line of care for high-risk patients28. In the Brazilian context, the Brazilian Association of Surgical Center, Anesthesia Recovery and Material and Sterilization Center Nurses (SOBECC) also recommends the use of support technologies as an essential preventive measure in critically ill patients in the ICU29.
Another resource identified in the reviewed studies was photographic documentation, used as a strategy to increase diagnostic accuracy and reliability in the classification of pressure ulcers. International literature demonstrates that standardized clinical photography increases the reproducibility of assessment among different professionals, reduces the risk of underreporting, and favors nursing education and research30,31. In Brazil, this resource can be incorporated into the Nursing Process (NP), in accordance with COFEN Resolution No. 736/2024, qualifying clinical records and strengthening the nurse's decision-making32. Thus, in addition to being a diagnostic resource, photography is configured as an instrument of standardization and safety, allowing greater traceability of care practices.
Nevertheless, the included studies showed significant heterogeneity in the adoption of these technologies, both in terms of the type of support surface and the systematization of photographic recording. This gap may be related to structural differences between hospitals, limited resources in regional services, and the absence of specific national protocols on the use of pressure ulcer prevention technologies. Brazilian research indicates that the unavailability of equipment, coupled with a lack of professional training for the proper use of resources, compromises the effectiveness of prevention 33,34. Thus, although there is robust evidence that special surfaces and photographic recording improve care, the practical applicability of these technologies in Brazil still requires greater institutional investment and standardization policies.
Training and Complementary Care
The training of the nursing team has been identified as one of the pillars for the prevention of pressure ulcers, especially in the critical care environment, where the complexity of care requires constant updating. The literature reinforces that periodic training, practical workshops, and awareness activities increase the team's adherence to preventive measures, strengthening the patient safety culture32,33. In Brazil, the National Patient Safety Program (PNSP), established by the Ministry of Health, recommends that the training of professionals be directly linked to institutional strategies for the prevention of adverse events, including pressure ulcers 34. Thus, continuous training should be understood not only as a one-off activity, but as a structuring axis of quality care.
In the Brazilian context, the National Policy on Permanent Education in Health (PNEPS) highlights the importance of learning in daily work, encouraging reflective and interactive practices that integrate theory and practice 35. For pressure ulcer prevention, Continuing Health Education (CHE) can address topics such as: proper application of the Braden scale and alternative instruments, repositioning techniques, microclimate management, skin care, prevention of injuries associated with medical devices, and correct use of support surfaces. National studies demonstrate that structured continuing education programs promote behavioral changes in the team, increase adherence to institutional protocols, and significantly reduce the incidence of pressure ulcers in the ICU 36,37.
In addition to training, the reviewed studies highlighted essential complementary care for preventive practice, such as skin hydration, application of protective barriers in at-risk areas, systematic inspection of skin integrity, monitoring for early signs of injury, and detailed clinical documentation of care provided. These complementary measures are widely recommended by international guidelines 28,38 and strengthen evidence-based care practice. Therefore, professional training, combined with complementary care, is a central element in consolidating safe, continuous, and effective practice.
Risk Prediction Scales
The Braden scale was the most cited among the studies included in this review, being widely used in health services due to its ease of application and international recognition. However, evidence suggests that its isolated use may not be sufficient in critically ill populations, as it presents low sensitivity in patients with specific conditions, such as trauma-surgical and neurological patients 36. In this sense, alternative scales, such as the Jackson and Cubbin scales, have demonstrated better risk discrimination capacity in critically ill patients 39.
International literature also highlights the Escala de Valoración Actual del Riesgo de desarrollar Úlceras por presión en Cuidados Intensivos (EVARUCI) as a more sensitive instrument for the ICU setting, especially because it includes variables related to the patient's clinical status and hemodynamic conditions (42). Brazilian studies corroborate the importance of adapting instruments to the profile of the population served, reinforcing that the inappropriate choice of scale can compromise care planning (40,41).
Thus, although the EB is widely adopted, the results of this review suggest the need to incorporate complementary or adapted scales for specific contexts of high complexity. This finding aligns with guidelines from the Registered Nurses’ Association of Ontario (RNAO), which recommends the judicious use of validated instruments and continuous reassessment of risk during hospitalization 38.
Institutional and multidisciplinary strategies
The studies analyzed demonstrated that institutional strategies, such as early skin assessment, structured repositioning, and the use of protective barriers, were decisive in reducing the incidence of pressure ulcers. These findings are aligned with the NPIAP and EPUAP guidelines, which consider such practices as high-impact interventions in prevention28. In Brazil, similar recommendations are described by the National Health Surveillance Agency (ANVISA), which highlights the importance of systematized clinical protocols and internal audits for monitoring the quality of care 42.
Another relevant point was the implementation of medical record audits and quality improvement projects, identified as strategies to increase team adherence to best practices. International studies demonstrate that regular audits and continuous feedback contribute to modifying clinical practices and improving prevention indicators 43. In the Brazilian context, experiences with the implementation of institutional patient safety protocols have revealed a positive impact on the reduction of pressure ulcers, highlighting the need for coordination between managers, care teams, and hospital quality centers 44,45.
Finally, the reviewed literature shows that multidisciplinary involvement is indispensable for the effectiveness of preventive strategies. Nurses, nursing technicians, nutritionists, physiotherapists, occupational therapists, and physicians play complementary roles, such as monitoring skin integrity, early mobilization, and adaptation of devices. Recent reviews reinforce that joint and interdisciplinary action results in better clinical outcomes, while fragmentation of care increases the vulnerability of the critically ill patient 46,47.
Impacts of Interventions in Clinical Practice
The studies included in this review showed that the implementation of structured prevention protocols resulted in a significant increase in team adherence to repositioning, from 55% to 89%, in addition to reducing the intervals between position changes. These results demonstrate that the application of clinical protocols not only improves the standardization of care but also promotes greater integration among professionals. International evidence corroborates this finding, highlighting that systematic adherence to prevention bundles is directly associated with a reduction in pressure ulcers in critically ill patients 43,48.
Another relevant impact was the improvement in the perception of teamwork, reported by nursing staff after the implementation of preventive strategies. This finding reinforces the notion that pressure ulcer prevention is not just a technical practice, but a process that requires interdisciplinary cooperation and effective communication among professionals. Recent research confirms that strengthening teamwork increases patient safety and reduces care errors 46,49. Therefore, the results of this study indicate that the adoption of protocols has both clinical and organizational effects, favoring a safer care environment.
Furthermore, a significant reduction in the incidence of pressure ulcers was observed over the evaluated periods, with particular emphasis on injuries related to medical devices, which represented 73.2% of occurrences. This finding is consistent with the current position of the NPIAP, which recognizes pressure ulcers associated with medical devices as a distinct category with high prevalence in high-complexity settings 28,50. Brazilian literature also reinforces the need for specific protocols for this type of injury, including regular inspection of contact areas, device fitting, and the use of protective dressings 51.
Key elements for effective prevention
The synthesis of the findings of this review reinforces that the prevention of pressure ulcers in the ICU depends on the combination of multiple factors, among which the following stand out: early risk assessment, microclimate management, structured repositioning, and continuous monitoring of skin integrity. These key elements are in line with the WHO Global Patient Safety Action Plan 2021–2030, which recognizes pressure ulcer prevention as an indicator of quality of care and patient safety 41. Furthermore, recent systematic reviews indicate that the implementation of bundles integrating these components significantly reduces the prevalence of pressure ulcers in critically ill patients 47,48.
Another key point identified was the importance of integrated multidisciplinary action. The involvement of different professional categories proved essential for the implementation of early mobilization measures, adaptation of devices, and monitoring of skin condition. Evidence confirms that interdisciplinary cooperation is associated with lower rates of skin-related complications and better clinical outcomes 46,49. In Brazil, ANVISA also emphasizes the need for interprofessional coordination to ensure comprehensive care and optimize available resources 42.
Finally, it is highlighted that the effectiveness of preventive strategies depends on the early recognition of individual and institutional risk factors, associated with the adoption of evidence-based practices. Brazilian literature indicates that underreporting, fragmentation of clinical records, and the absence of continuous monitoring are still barriers to the advancement of this agenda 51,52. Thus, it becomes indispensable that health institutions adopt prevention policies supported by evidence-based protocols, continuing education, and audit mechanisms, consolidating pressure ulcer prevention as a care priority and ethical commitment of nursing.
The following is a comparison between the main results of the integrative review and the current evidence from the scientific literature (Chart 4).
Chart 4 - Comparison between the main findings of the review and the evidence from the scientific literature. Garanhuns, Pernambuco, Brazil, 2025.
|
Category |
Review findings |
Literature |
|
Technologies and resources |
Support surfaces (foam, gel, alternating air); photographs for evaluation; dressings under devices. |
They recommend use as a first line 28,38. They highlight dressings on devices 51. |
|
Training and complementary care |
Team training; repositioning; increased adherence following protocols. |
They reinforce the impact of lifelong learning27,28. |
|
Risk prediction scales |
Braden predominated; Jackson, Cubbin, and Evaruci showed greater sensitivity in the ICU. |
They confirm the limitations of the Braden scale alone and the greater accuracy of specific scales41,42. |
|
Institutional and multi-professional strategies |
Early assessment, structured repositioning, skin barriers, audits. |
They reinforce protocols, audits, and multidisciplinary involvement. 29. |
|
Impacts on clinical practice |
Adherence to repositioning ↑ (55% → 89%); reduction in the incidence of pressure ulcers (OR=0.41). |
They demonstrate that prevention bundles are effective 50. |
|
Profile and prevalence of lesions |
15.4% developed pressure ulcers; the majority (73.2%) were associated with devices. |
They classify pressure ulcers caused by devices as a distinct and prevalent category 28,51. |
|
Key elements for effective prevention |
Early recognition, microclimate control, use of scales, multi-professional integration. |
They emphasize the role of the nurse and teamwork in patient safety. 32. |
Source: Authors' own work, 2025.
FINAL CONSIDERATIONS
This integrative review identified that nursing care for pressure ulcer prevention in Intensive Care Units requires the articulation of different strategies, including support technologies, team training, judicious use of predictive scales, institutional protocols, and integrated multidisciplinary action. However, some limitations should be highlighted.
The methodological heterogeneity among the studies, the variation in care contexts (small, regional, and referral hospitals), and the lack of standardization in interventions hinder direct comparison between findings and limit the generalization of results. Furthermore, a scarcity of recent national studies was observed, reinforcing the need for multicenter research in Brazil that evaluates the effectiveness of protocols and technologies in different hospital settings.
Another important limitation refers to the predominance of observational studies and secondary reviews, which, although providing relevant evidence, have limitations regarding the establishment of causal relationships. The absence of robust randomized clinical trials, especially in Latin American countries, compromises the production of more solid recommendations. International literature also recognizes these gaps and emphasizes the importance of greater investment in interventional research in the field of pressure ulcer prevention, with a special focus on injuries related to medical devices.
From the perspective of implications for nursing practice, the results of this review reinforce the centrality of the nurse in the planning, implementation, and evaluation of pressure ulcer prevention strategies in critically ill patients. The integration of photographic documentation, the use of more sensitive scales for the ICU environment, the incorporation of multidisciplinary protocols, and continuing health education emerge as indispensable measures to improve the quality of care. In Brazil, such practices should be aligned with public patient safety policies, such as the National Patient Safety Program (PNSP), and the regulations of the Federal Nursing Council, especially COFEN Resolution No. 736/2024, which reinforces the importance of the Nursing Process in the prevention of complications.
Therefore, the implications of this review indicate that pressure ulcer prevention should be understood not only as a set of isolated techniques, but as a complex, ethical, and interdisciplinary practice, supported by scientific evidence and the coordinated action of different healthcare professionals. The consolidation of protocols adapted to the Brazilian reality, coupled with the strengthening of continuing education and institutional investment in prevention technologies, constitutes an essential path to reducing the incidence of pressure ulcers in ICUs and ensuring greater quality and safety in the care provided.
REFERENCES
1. Silva MA. Riscos no ambiente hospitalar: uma revisão de literatura. Rev Bras Enferm. 2017;70(2):367-373. doi: https://doi.org/10.1590/0034-7167-2016-0479
2. Girão AA, Melo GAA, Lima JB, Silva VL, Vasconcelos GIO, Caetano JA. Complicações infecciosas e a evolução para sepse em pacientes com lesões por pressão em UTI. Rev Bras Ter Intensiva. 2020;32(2):156-162. doi: https://doi.org/10.5935/0103-507X.20200027
3. Silva LM, Oliveira AC, Nogueira LMV, Costa IKF, Torres GV. Prevenção de lesões por pressão em unidades de terapia intensiva: práticas e desafios. Enferm Foco. 2019;10(1):45-52. doi: https://doi.org/10.21675/2357-707X.2019.v10.n1.1760
4. National Pressure Ulcer Advisory Panel. National pressure ulcer advisory panel support surface standards initiative 2016 [Internet]. Washington (DC): NPUAP; 2016 [cited 2024 Jun 18]. Available from: https://sobest.com.br/wp-content/uploads/2020/10/CONSENSO-NPUAP-2016_traducao-SOBEST-SOBENDE.pdf
5. Instituto Brasileiro para Segurança do Paciente. 7 passos essenciais no manejo de pacientes para prevenção de lesão por pressão [Internet]. 2017 [cited 2024 Aug 25]. Available from: https://www.segurancadopaciente.com.br/qualidade-assist/7-passos-essenciais-no-manejo-de-pacientes-para-prevencao-de-lesao-por-pressao/
6. Li Z, Lin F, Thalib L, Chaboyer W. Global prevalence and incidence of pressure injuries in hospitalized adult patients: a systematic review and meta-analysis. Int J Nurs Stud. 2020;105:103546. doi: https://doi.org/10.1016/j.ijnurstu.2020.103546
7. Ministério da Saúde (BR). Relatórios de incidentes relacionados à assistência à saúde: dados epidemiológicos de lesões por pressão em unidades de terapia intensiva, 2014-2021 [Internet]. Brasília-DF: Ministério da Saúde; 2021. [cited 2024 Jul 1]. Available from: https://www.gov.br/anvisa
8. Smaniotto MC, Ribeiro MC, Richter SA, Quadros A. Conhecimento da equipe de enfermagem na prevenção de lesão por pressão no ambiente hospitalar. Rev Enferm Atual In Derme. 2022;96:e021234. doi: https://doi.org/10.31011/reaid-2022-v.96-n.34-art.1374
9. Xavier DCB, Ferreira RC, Lima J. O enfermeiro na assistência e prevenção das lesões por pressão. Braz J Health Rev. 2023;6:479-490. doi: https://doi.org/10.34119/bjhrv6n1-039
10. Rodrigues CA, Lacerda MR, Lopes LM, Nascimento ERP, Bernardes RM, Zagonel IPS. Desafios da prevenção de lesões por pressão em unidades de terapia intensiva. Rev Lat Am Enfermagem. 2019;27:e3137. doi: https://doi.org/10.1590/1518-8345.2864.3137
11. Oliveira RF, Souza JP. Fatores de risco e prevenção de lesões por pressão em pacientes de UTI. Rev Bras Enferm. 2020;73(4):e20180999. doi: https://doi.org/10.1590/0034-7167-2018-0999
12. Mendes KDS, Silveira RCCP, Galvão CM. Uso de gerenciador de referências bibliográficas na seleção dos estudos primários em revisão integrativa. Texto Contexto Enferm. 2019;28:e20170204. doi: https://doi.org/10.1590/1980-265X-TCE-2017-0204
13. Peters MDJ, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. JBI Evid Implement. 2015;13(3):141-46. doi: https://doi.org/10.1097/XEB.0000000000000050
14. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi: https://doi.org/10.1136/bmj.n71
15. Tortora GJ, Derrickson BH. Princípios de anatomia e fisiologia. 15ª ed. Rio de Janeiro: Guanabara Koogan; 2017.
16. Vestemberg CV, Almeida FC, Paixão GM. Prevenção de lesão por pressão no contexto hospitalar: uma revisão sistemática. Rev CPAQV. 2023;15(1):e15n1-10R. doi: https://doi.org/10.36692/V15n1-10R
17. Higgins J, Casey S, Taylor E, Wilson R, Halcomb P. Comparing the Braden and Jackson/Cubbin pressure injury risk scales in trauma-surgery ICU patients. Crit Care Nurse. 2020;40(6):52-61. doi: https://doi.org/10.4037/ccn2020874
18. Levido A, Fulbrook P, Barakat-Johnson M, Campbell J, Delaney L, Latimer S, et al. Pressure injury prevention practice in Australian intensive care units: a national cross-sectional survey. Aust Crit Care. 2023;36(2):186-94. doi: https://doi.org/10.1016/j.aucc.2021.11.004
19. Almeida AGA, Pascoal LM, Rolim ILTP, et al. Relação entre o diagnóstico risco de lesão por pressão e a escala de Braden. Rev Enferm UERJ. 2021;29:e61666. https://doi.org/10.12957/reuerj.2021.61666
20. Moser CH, Peeler A, Long R, Schoneboom B, Budhathoki C, Pelosi P, et al. Prevention of endotracheal tube-related pressure injury: a systematic review and meta-analysis. Am J Crit Care. 2022;31(5):416-24. doi: https://doi.org/10.4037/ajcc2022644
21. Turmell M, Cooley A, Yap TL, Alderden J, Sabol VK, Lin JA, et al. Improving pressure injury prevention by using wearable sensors to cue critical care patient repositioning. Am J Crit Care. 2022;31(4):295-305. doi: https://doi.org/10.4037/ajcc2022701
22. Coyer F, Cook JL, Doubrovsky A, Campbell J, Vann A, McNamara G, et al. Implementation and evaluation of multilayered pressure injury prevention strategies in an Australian intensive care unit setting. Aust Crit Care. 2022;35(2):143-52. doi:https://doi.org/10.1016/j.aucc.2021.03.005
23. Jesus WG, Matheus FAV, Silva MG, Peixoto TM, Oliveira FGV, Oliveira JRN, et al. Assistência de enfermagem e fatores de risco na prevenção de lesão por pressão. Rev Nursing. 2023;26(302):9779-9786. doi: https://doi.org/10.36489/nursing.2023v26i302p9779-9786
24. Soares FM, Vieira TV, Mazocoli E, Souza RC. Instrumentos preditores de risco para lesão por pressão em pacientes críticos. Acta Paul Enferm. 2023;36:eAPE008032. doi: https://doi.org/10.37689/acta-ape/2023AO008032
25. Sichieri K, Matos TM, Santos TR, Secoli SR. Prevenção de lesão por pressão em unidade de terapia intensiva: implementação de melhores práticas. Rev Gaucha Enferm. 2024;45:e20240166. doi: https://doi.org/10.1590/1983-1447.2024.20240166
26. Buffon MR, Severo IM, Azzolin KO, Lucena AF. Incidência de lesão por pressão em pacientes críticos com e sem COVID-19: estudo de coorte. Rev Gaucha Enferm. 2024;45:e20230221. doi: https://doi.org/10.1590/1983-1447.2024.20230221
27. Ribeiro RN, Oliveira DV, Paiva WS. Incidence of pressure injury in patients with moderate and severe traumatic brain injury: a systematic review. BMJ Open. 2024;14:e089243. doi: https://doi.org/10.1136/bmjopen-2024-089243
28. National Pressure Injury Advisory Panel, European Pressure Ulcer Advisory Panel, Pan Pacific Pressure Injury Alliance. Prevention and treatment of pressure ulcers/injuries: clinical practice guideline. 3rd ed. 2019.
29. Associação Brasileira de Enfermeiros de Centro Cirúrgico. Diretrizes de práticas seguras em enfermagem perioperatória. 7ª ed. São Paulo: SOBECC; 2022.
30. Langemo DK, Anderson J, Hanson D, Hunter S, Thompson P. Photographic wound assessment tool: validity and reliability. J Wound Ostomy Continence Nurs. 2018;45(1):14-22. doi: https://doi.org/10.1097/01.ASW.0000431329.50869.6f
31. Milne SD, Connolly P. The use of smartphone applications in wound assessment: an international survey. J Wound Care. 2020;29(8):454-60. doi: https://doi.org/10.1177/1534734619853916
32. Conselho Federal de Enfermagem (BR). Resolução nº 736, de 17 de janeiro de 2024. Dispõe sobre o processo de enfermagem. Brasília-DF: COFEN; 2024.
33. Dantas ALM, Costa IKF, Nóbrega WG, Torres GV. Estratégias de prevenção de lesões por pressão em terapia intensiva: revisão integrativa. Rev Enferm UFPE. 2021;15:e247281. doi: https://doi.org/10.5205/1981-8963-v11i5a23344p1943-1952-2017
34. Souza TS, Silva GRF, Nogueira GA, Oliveira KMC. Barreiras para implementação de medidas preventivas de lesões por pressão em hospitais brasileiros. Rev Bras Enferm. 2022;75(1):e20210045. doi: https://doi.org/10.1590/1980-265X-TCE-2023-0396pt
35. Beeckman D, Schoonhoven L, Fletcher J, Furtado K, Heyman H, Paquay L, et al. Pressure ulcers and incontinence-associated dermatitis: effectiveness of prevention interventions. Int J Nurs Stud. 2020;104:103512. doi: https://doi.org/10.1016/j.ijnurstu.2019.103512
36. Lima AFC, Castilho V, Baptista CMC, Rogenski NMB. Educação continuada e lesões por pressão em UTI: impacto de estratégias educativas. Acta Paul Enferm. 2019;32(2):191-198. doi: https://doi.org/10.1590/0034-7167-2018-0778
37. Brasil. Portaria nº 529, de 1º de abril de 2013. Institui o Programa Nacional de Segurança do Paciente. Brasília-DF: Ministério da Saúde; 2013.
38. Ministério da Saúde (BR). Política nacional de educação permanente em saúde: o que se tem produzido para o seu fortalecimento? Brasília-DF: Ministério da Saúde; 2018.
39. Barbosa TP, Beccaria LM, Poletti NAA. Educação permanente para prevenção de úlcera por pressão: impacto em indicadores de qualidade. Texto Contexto Enferm. 2020;29:e20180442. doi: https://doi.org/10.26694/reufpi.v13i1.4238
40. Registered Nurses’ Association of Ontario. Assessment and management of pressure injuries for the interprofessional team. 4th ed. Toronto: RNAO; 2024.
41. Cox J. Predictive power of the Braden scale for pressure sore risk in adult critical care patients: a comprehensive review. J Wound Ostomy Continence Nurs. 2021;48(2):120-26. doi: https://doi.org/10.1097/won.0b013e31826a4d83
42. Falcão LM, Oliveira BML, Santos JF. Validação da escala EVARUCI em pacientes críticos. Rev Lat Am Enfermagem. 2023;31:e3854. doi: https://doi.org/10.26694/reufpi.v13i1.4238
43. Moore Z, Patton D. Risk assessment tools for the prevention of pressure ulcers. Cochrane Database Syst Rev. 2019;(1):CD006471. Doi: https://doi.org/10.1002/14651858.cd006471.pub4
44. Agência Nacional de Vigilância Sanitária (BR). Assistência segura: uma reflexão teórica aplicada à prática. Brasília: ANVISA; 2017.
45. Tayyib N, Coyer F, Lewis P. Implementing a pressure ulcer prevention bundle in adult intensive care. Int Wound J. 2016;13(5):912-921. doi: https://doi.org/10.1016/j.iccn.2016.04.005
46. Ministério da Saúde (BR). Protocolo básico de segurança do paciente: prevenção de lesão por pressão. Brasília-DF: Ministério da Saúde; 2017.
47. Barbosa TP, Beccaria LM, Poletti NAA. Impacto da implementação de protocolos de prevenção de lesão por pressão em indicadores assistenciais. Rev Gaucha Enferm. 2021;42:e20200312. Doi: https://doi.org/10.1590/1983-1447.2024.20240166.pt
48. Chaboyer W, Bucknall T, Webster J, McInnes E, Banks M, Wallis M, et al. Teamwork and patient safety in intensive care units: a multicenter study. Int J Nurs Stud. 2021;115:103868. doi: https://doi.org/10.3233/SHTI220120
49. Lavallée JF, Gray TA, Dumville J, Cullum N. The effectiveness of care bundles in preventing pressure ulcers: a systematic review and meta-analysis. Implement Sci. 2019;14(1):51. doi: https://doi.org/10.2174/1874434602115010074
50. Niederhauser A, VanDeusen Lukas C, Parker V, Ayello EA, Zulkowski K, Berlowitz D. Comprehensive programs for preventing pressure ulcers: a review of the literature. Adv Skin Wound Care. 2020;33(3):123-36. doi: https://doi.org/10.1016/j.iccn.2016.04.005
51. Black JM, Cuddigan JE. Medical device-related pressure injuries: NPIAP position statement. J Wound Ostomy Continence Nurs. 2021;48(3):187-90. doi: https://doi.org/10.1111/jocn.15682
Funding and Acknowledgments:
This research received no funding.
Data Availability Statement:
No databases were generated in this study. The information presented is described in the body of the article.
Conflict of Interest Statement:
Nothing to declare.
Author Contributions:
José Macêdo de Almeida: manuscript writing, data acquisition, analysis and interpretation, and study planning.
Belarmino Santos de Sousa Júnior: research guidance, project corrections, and final approval of the version.
Bárbara Maria Lopes da Silva Brandão: general research guidance and writing corrections.
Karyne Kirley Negromonte Gonçalves: general research guidance and writing corrections.
Thaíse Alves Bezerra: general research guidance and writing corrections.
Scientific Editor: Ítalo Arão Pereira Ribeiro. Orcid: https://orcid.org/0000-0003-0778-1447
Rev Enferm Atual In Derme 2026;100(1): e026027
![]()