INTEGRATIVE REVIEW
EVIDENCE ON TREATMENT OF LYMPHEDEMA AND
CUTANEOUS AND BLISTERING LESIONS ASSOCIATED WITH ERYSIPELAS
EVIDÊNCIAS SOBRE TRATAMENTO DO LINFEDEMA E LESÕES CUTÂNEAS
E BOLHOSAS ASSOCIADAS À ERISIPELA
EVIDENCIAS SOBRE
TRATAMIENTO DEL LINFEDEMA
Y LESIONES CUTÁNEAS Y BULLOSAS ASOCIADAS A ERISIPELA
https://doi.org/10.31011/reaid-2026-v.100-n.2-art.2729
¹Larissa Fernandes da
Silva Oliveira
²Melka Maria Frazão de
Souza
³Paulo Geovane Pestana Pinheiro
⁴Francisco Carlos
Costa Magalhães
⁵Mayra Sharlenne
Moraes Araújo
⁶Tamires Barradas
Cavalcante
1Graduanda em Enfermagem-UFMA. Pinheiro –Maranhão, Brazil.
ORCID: https://orcid.org/0009-0000-5537-792X.
2 Graduanda em Enfermagem-UFMA. Pinheiro
– Maranhão, Brazil. ORCID: https://orcid.org/0009-0003-4964-9660.
3 Graduando em Enfermagem-UFMA. Pinheiro –Maranhão, Brazil.
ORCID: https://orcid.org/0000-0002-4405-5674.
4 Enfermeiro. Mestre em Ciências da
Saúde. Docente do Centro de Ciências de Pinheiro- UFMA. São Luís – Maranhão,
Brazil. ORCID: https://orcid.org/0000-0002-9454-760X.
5Enfermeira. Doutora em
Saúde Coletiva. Docente do Centro de Ciências de Pinheiro- UFMA. São Luís –
Maranhão, Brazil. ORCID: https://orcid.org/0000-0002-9769-834X.
6Enfermeira. Doutora em Saúde
Coletiva. Docente do Centro de Ciências de Pinheiro- UFMA. São Luís – Maranhão,
Brazil. ORCID: https://orcid.org/0000-0002-4063-533X
Corresponding
Author
Larissa Fernandes da
Silva Oliveira
Rua Capitão João Moraes,
Alcântara, 740. CEP 65200-000–Pinheiro –MA, Brazil. contact: +55 91 99234-2904.
E-mail: larissafernandes72414@gmail.com
Submission: 04-02-2026
Approval: 20-03-2026
ABSTRACT
Introduction: Lymphedema related to erysipelas is a condition caused
by the accumulation of lymph, skin alterations, and recurrent infections, with
possible formation of blistering lesions that compromise the function of the
affected limb. Objective: To
analyze the evidence on the treatment of lymphedema related to the development
of skin and blistering lesions in patients with erysipelas. Method: This
is an integrative, exploratory, and descriptive review with a
qualitative e approach, involving searches in national and international
databases, selection of studies published between 2015 and 2025, standardized
data extraction, and analysis through interpretative synthesis. Results: Ten
studies were included, which addressed surgical, pharmacological, compressive,
physiotherapeutic, and care interventions; combined therapies such as
liposuction followed by continuous compression, lymphatic drainage,
standardized protocols, and the use of pharmacological agents, which were
associated with reduced edema, lower recurrence of erysipelas, and improved skin integrity. Discussion: The management of
lymphedema with cutaneous and blistering lesions in erysipelas involves
combined strategies, such as antibiotic therapy, compressive therapies, skin
care, and multidisciplinary follow-up. Standardized clinical protocols and
continuous monitoring highlight the role of nursing in preventing recurrences,
caring for lesions, and promoting treatment adherence. Adjuvant and integrative
approaches are also identified as complementary alternatives. Final considerations: Management
requires continuous interdisciplinary care, with nursing playing a central
role in prevention, monitoring, and health education, and there is a need for increased production of primary studies on
professional practice.
Keywords: Erysipelas; Skin ulcer; Blister;
Lymphedema; Nursing Care.
RESUMO
Introdução: O linfedema relacionado à erisipela é uma condição
determinada pelo acúmulo de linfa, alterações cutâneas e infeções recorrentes,
com possíveis formações de lesões bolhosas que comprometem a função do membro
acometido. Objetivo: Analisar as evidências sobre o tratamento do
linfedema relacionado ao desenvolvimento de lesões cutâneas e bolhosas em
pacientes com erisipela. Método: Trata-se de uma revisão integrativa,
exploratória e descritiva com abordagem qualitativa com buscas em bases
nacionais e internacionais, seleção de estudos publicados entre 2015 e 2025,
extração padronizada e análise por síntese interpretativa. Resultados: Dez
estudos foram incluídos, no qual abordaram intervenções cirúrgicas,
farmacológicas, compressivas, fisioterapêuticas e medidas de cuidado; terapias
combinadas, como lipoaspiração seguida de compressão contínua, drenagem
linfática, protocolos padronizados e uso de agentes farmacológicos que se
associaram à redução do edema, menor recorrência de erisipela e melhora da integridade
cutânea. Discussão: O manejo do linfedema com lesões cutâneas e bolhosas
em erisipela envolve estratégias combinadas, como antibioticoterapia, terapias
compressivas, cuidados com a pele e acompanhamento multiprofissional.
Protocolos clínicos padronizados e monitoramento contínuo destacam o papel da
enfermagem na prevenção de recidivas, cuidado das lesões e promoção da adesão
ao tratamento. Abordagens adjuvantes e integrativas também são apontadas como
alternativas complementares. Considerações finais: O manejo exige
cuidado interdisciplinar contínuo, com papel central da enfermagem na
prevenção, monitorização e educação em saúde, e demanda maior produção de
estudos primários sobre a atuação profissional.
Palavras-chave:
Erisipela; Avulsões Cutâneas; Vesícula; Linfedema; Cuidados de Enfermagem.
RESUMEN
Introducción: El linfedema relacionado con la erisipela es una
condición determinada por la acumulación de linfa, alteraciones cutáneas e
infecciones recurrentes, con posibles formaciones de lesiones ampollosas que
comprometen la función del miembro afectad.. Objetivo Analizar la
evidencia sobre el tratamiento del linfedema relacionado con el desarrollo de
lesiones cutáneas y ampollosas en pacientes
con erisipela. Método: Se trata de una revisión
integradora, exploratoria y descriptiva
con enfoque cualitativo, con búsquedas en bases nacionales e internacionales,
selección de estudios publicados entre 2015 y 2025, extracción estandarizada y
análisis mediante síntesis interpretativa. Resultados: Se incluyeron
diez estudios, los cuales abordaron intervenciones quirúrgicas, farmacológicas,
compresivas, fisioterapéuticas y medidas de cuidado; terapias combinadas, como
liposucción seguida de compresión continua, drenaje linfático, protocolos
estandarizados y uso de agentes farmacológicos que se asociaron con la reducción
del edema, menor recurrencia de erisipela y mejora de la integridad cutánea. Discusión:
El manejo del linfedema con lesiones
cutáneas y ampollosas en erisipela implica estrategias combinadas, como la
antibioticoterapia, las terapias compresivas, el cuidado de la piel y el
seguimiento multiprofesional. Los protocolos clínicos estandarizados y la
monitorización continua destacan el papel de la enfermería en la prevención de
recaídas, el cuidado de las lesiones y la promoción de la adherencia al tratamiento.
También se señalan enfoques adyuvantes e integrativos como alternativas
complementarias. Consideraciones
finales: El manejo exige un cuidado interdisciplinario
continuo, con un papel central de la enfermería en la prevención,
monitorización y educación en salud, y demanda una mayor producción de estudios
primarios sobre la actuación profesional.
Palabras clave: Erisipela; Lesiones por Desenguantamiento; Vesícula; Linfedema; Atención de Enfermería.
INTRODUCTION
Erysipelas is a bacterial infection that
affects the superficial layer of the skin, causing high inflammation of the
lymphatic vessels, with β-hemolytic Streptococcus being the main causative
agent(1). Among the main risk factors associated with the
development of the disease are advanced age, diabetes, and reduced immunity(2).
In this perspective, the clinical picture of erysipelas usually manifests
suddenly, presenting high fever in the first 12 to 24 hours, accompanied by the
appearance of a well-defined, hot, painful, edematous, erythematous plaque,
generally located on one of the lower limbs(3).
Lymphedema is a chronic condition
characterized by an increase in the volume of soft tissues in the affected
area, which can progress to significant deformities(4). Therefore,
the affected limb becomes voluminous, edematous, heavy, and painful. As the
disease progresses, patients develop recurrent infections and non-healing
wounds, thus requiring intensive care(5).
Furthermore, complications can also
include skin changes, which initially appear as a localized area of redness and
swelling, but gradually progress, presenting intensely red, raised borders that
are clearly separated from the surrounding healthy tissue(6). Thus,
when the condition worsens, blisters, wounds, and lymphedema may appear(7).
Bullous manifestation is usually more common in women and in individuals with
hepatic or renal impairment. In these cases, the presence of blisters is
related to a higher chance of infection by methicillin-resistant Streptococcus
aureus strains(6).
From this perspective, it is evident
that erysipelas can develop into an intense inflammatory process, leading to
damage to the lymphatic vessels. This damage can result in the development of
lymphedema, where the accumulation of lymphatic fluid causes swelling and
increased volume in a specific region of the body. Lymphedema, in turn, creates
a favorable environment for the development of skin and bullous lesions, as the
increased pressure on tissues due to swelling can damage the skin, making it
more vulnerable to wounds, ulcers, and blisters. In line with this, an
integrated treatment approach, including infection control and skin care, is
crucial for managing these conditions and improving the quality of life of
affected patients.
Thus, this study aimed to investigate
and analyze the available evidence on the treatment of lymphedema associated
with the development of skin and bullous lesions in patients with erysipelas,
seeking to improve the efficiency of therapeutic interventions and enhance the
quality of life of patients.
METHODS
This is an integrative literature review,
exploratory and descriptive in nature, with a qualitative approach. Thus, an
integrative review is characterized as a research method that allows for the
systematic and organized union and synthesis of findings from different studies
on a specific topic or question, providing a deeper understanding of the
subject(8).
The guiding questions, as well as the
problem formulated in interrogative format, are developed throughout the body
of the study with the aim of clarifying them, rigorously following the
established scientific path(9). In this sense, for the formulation
of the guiding question of this review, the PICo strategy (Population, Interest
and Context) was used, whose structure was based on the identification of the
central elements of the investigated problem, such as: erysipelas, lymphedema,
cutaneous avulsions, treatment. Therefore, through these, the question was
defined: "What is the evidence on the treatment of lymphedema associated
with the development of cutaneous and bullous lesions in patients with
erysipelas?".
Furthermore, the literature search
process is a central element for the quality of evidence synthesis, so the
effectiveness of this step directly influences the final result of the study(10).
From this perspective, the sample set was fitted with descriptors defined from
the standardized vocabularies Health Sciences Descriptors (DeCS) and Medical
Subject Headings (MeSH) together with the Boolean operators AND and OR, whose
suitability for the review resulted in: P ("Erysipelas") AND I
("Skin ulcer" OR "Skin Diseases" OR "Blister" OR
"Lymphedema") AND Co ("Therapy" OR "Treatment
Outcome" OR "Nursing Care" OR "Cost of Illness"), in
order to ensure greater precision in retrieving relevant studies.
After
defining the suitable and unsuitable descriptors, the search was carried out in
the selected databases. The identification of studies available in national and
international journals took place between May 2025 and June 2025, using the
following databases: Virtual Health Library (BVS), Google Scholar, Lilacs,
PubMed, ScienceDirect, and Web of Science. Selected full-text articles were
obtained electronically through the CAPES Journals Portal, with access
authenticated by the CAFe system, provided by the Federal University of
Maranhão (UFMA).
Chart 1 –
Databases and descriptors used to identify the studies
|
Database
|
Descriptors
|
|
BVS
|
(“Erisipela”) AND (“avulsões cutâneas” OR “dermatopatias” OR “vesícula” OR “Linfedema”) AND (“Terapia” OR “Tratamento” OR
“Cuidados de enfermagem” OR “Efeitos
Psicossociais da Doença”).
|
|
Google Scholar
|
("Erisipela") AND
("avulsões cutâneas" OR "dermatopatias"
OR "vesícula" OR "Linfedema") AND ("Terapia" OR "Tratamento" OR "Cuidados de
enfermagem"
OR "Efeitos Psicossociais da Doença").
|
|
Lilacs
|
("Erisipela") AND
("avulsões cutâneas" OR "dermatopatias"
OR "vesícula" OR "Linfedema") AND ("Terapia" OR "Tratamento" OR "Cuidados de
enfermagem"
OR "Efeitos Psicossociais da Doença").
|
|
Pubmed
|
(“Erysipelas”) AND (“Skin
ulcer” OR “Skin Diseases” OR “Blister” OR
“Lymphedema”) AND (“Therapy” OR “Treatment Outcome” OR “Nursing Care” OR “Cost of Illness”).
|
|
ScienceDirect
|
("Erysipelas")
AND ("Skin ulcer" OR "Skin Diseases" OR
"Blister" OR "Lymphedema") AND ("Therapy" OR "Treatment Outcome" OR "Nursing
Care" OR
"Cost of Illness").
|
|
Web of
Science
|
(“Erysipelas”) AND
(“Skin ulcer” OR “Skin Diseases” OR “Blister” OR “Lymphedema”) AND (“Therapy” OR “Treatment Outcome”
OR “Nursing
Care” OR
“Cost of Illness”).
|
Source: The authors, 2025.
Following the searches, the screening
and selection of articles was carried out, in accordance with the steps
recommended by the PRISMA (Preferred Reporting Items for Systematic Reviews and
Meta-Analyses) guidelines. The process began with the organization of the
references obtained from the databases, which were imported into the Rayyan
platform, an online tool developed specifically to support systematic reviews,
facilitating the management, screening, and exclusion of duplicates.
The titles and abstracts were read.
Then, the full texts of potentially eligible articles were read. After the
final selection of studies, systematic data extraction began, based on an
instrument adapted from the matrix proposed by Ursi (2005). This instrument
allowed for the standardized recording of essential information for each study,
such as title, year of publication, country of origin, type of research,
objectives, methodology, main results, and conclusions. Data analysis occurred
in three complementary stages: exploratory reading, analytical reading, and
interpretive synthesis.
This review included national and
international studies obtained from filters applied to databases. Publications
were selected, including reviews and original research, that presented primary
data on the treatment of lymphedema in patients with erysipelas, with an
emphasis on cases associated with cutaneous and bullous lesions. Only articles
available in full, published between 2015 and 2025, written in Portuguese,
English, or Spanish, peer-reviewed, and with methodological rigor compatible
with the study's objectives were considered.
Regarding exclusion criteria, articles
that did not directly address the treatment of lymphedema associated with
erysipelas; reviews without clear methodological criteria; opinion articles;
and publications classified as grey literature, such as theses, monographs, and
institutional reports, were disregarded because they did not undergo formal
peer review. Studies duplicated in the databases and those unavailable in full
text were also excluded. This standardization sought to ensure methodological
consistency and the reliability of the results obtained.
The PRISMA
2020 statement emphasizes that systematic reviews should describe in a
transparent and detailed manner the process of identifying and selecting
studies. It also highlights that the guidelines also recommend the use of a
flowchart that presents the steps of identification, screening, eligibility and
final inclusion of studies. Considering these guidelines, the following
flowchart was developed, which brings together all the steps of the study
selection process for this review(11).
Figure 1- Flowchart for
selecting included primary studies according to PRISMA
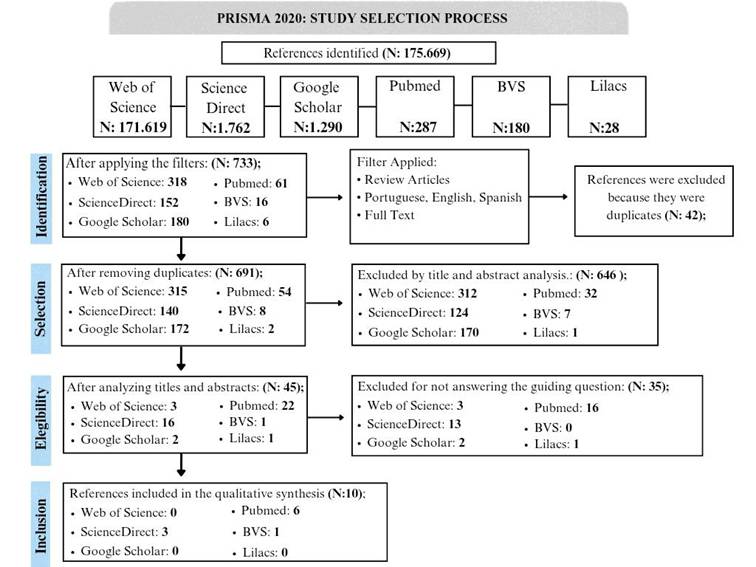
Source: Adapted and translated from PRISMA
(2020).
RESULTS
Based on the analysis of the studies, 10
articles met the inclusion criteria. Therefore, the results were structured in
two distinct stages. The first refers to the characterization of the included
studies, presented in Table 2, which contains information on the title,
origin/year of publication, objectives, methodology, and main results. The
second stage consists of a descriptive synthesis of the evidence found on the
treatment of lymphedema associated with the appearance of cutaneous and bullous
lesions in patients with erysipelas.
During the search, few specific
scientific publications from the nursing field on the subject were found. The
publications originated from the medical field, mainly in international
journals of plastic surgery, dermatology, and clinical medicine. Most of the
identified studies have an observational, descriptive, or narrative and
systematic review design, focused on the evaluation of therapeutic protocols
and pharmacological interventions. Regarding the origin of the studies, a
predominance of research published in European journals was observed,
particularly from Germany, France, Sweden, the Netherlands, and Portugal,
representing approximately 70% of the analyzed publications. Publications from
the United States and Ethiopia were also identified.
In terms of temporal distribution, the
included studies span the period from 2016 to 2025, with a higher concentration
of publications from 2020 onwards. As for the type of study, clinical review
articles and medical practice guidelines prevailed (57%), followed by
experimental and observational research (43%). The predominant area of
concentration was dermatology and reconstructive surgery.
The objectives of the studies included
the efficacy of combined therapies, such as liposuction associated with
controlled compression; the use of sodium selenite in patients with lymphedema
secondary to cancer associated with erysipelas; and the standardization of
clinical protocols for the diagnosis and management of lymphedema. Studies
focused on the antibacterial activity of plant extracts against microorganisms
isolated from wounds in patients with lymphedema were also identified.
The main results described effects
related to edema reduction and prevention of erysipelas recurrence, control of
skin infections, maintenance of lymphatic volume after surgical procedures, and
the effects of pharmacological interventions in clinical management. The S2k
guidelines, the French National Diagnosis and Care Protocol (PNDS), and the
Pediatric and Primary Lymphedema Working Group of VASCERN (VASCERN PPL)
presented standardized protocols with a multidisciplinary approach to
lymphedema management, including medical, physiotherapy, and psychological
follow-up of patients.
Chart 2 – Characterization of the
studies, title, origin/year, objectives, methodology, main results
|
Title
|
Origin/
Year
|
Objectives
|
Methodology
|
Main
Results
|
|
Sodium
selenite and cancer related lymphedem: Biological and Pharmacological
effects.15
|
Germany/
2016
|
To analyze
the effects of sodium selenite on cancer-related lymphedema and its
biological and therapeutic mechanisms.
|
Descriptive
study, based on clinical and experimental evidence on the use of sodium
selenite in patients with secondary lymphedema.
|
Sodium
selenite reduced the volume of lymphedema and the incidence of erysipelas,
with antioxidant and anti-inflammatory action, improving the response to
physiotherapy treatment.
|
|
Lymphedem:
Diagnostic workup and managemet.20
|
United
States/
2017
|
To present a
practical overview of the diagnosis and clinical management of lymphedema.
|
This
descriptive study, based on a review of scientific literature and recent
clinical evidence, is aimed at providing medical updates.
|
Diagnosis is
clinical and complemented by imaging tests. Treatment includes decongestive
therapy, lymphatic drainage, and compression, with surgery only in resistant
cases.
|
|
S2k guidelines for skin and soft Tissue
infections Excerpts from the S2k guidelines for “calculated initial
parenteral treatment
of bacterial infections in adults update
2018”.16
|
Germany/
2019
|
To
standardize the diagnosis and treatment of skin and bacterial infections,
focusing on initial antibiotic therapy and the rational use of
antimicrobials.
|
This is a
descriptive and qualitative study, specifically a systematic review with
expert consensus (Guideline S2k).
|
He
established protocols for skin infections, indicating penicillin for
erysipelas and cephalosporins for cellulitis. Severe cases require
broad-spectrum antibiotics and surgery.
|
|
Shaving Technique and Compression
Therapy for
Elephantiasis Nostras Verrucosa
(Lymphostatic
Verrucosis) of Forefeet and Toes in
End-Stage Primary
Lymphedema: A 5 Year Follow-Up Study in
28 Patients
and a Review of the Literature.13
|
Netherlands
/2020
|
To
evaluate the effectiveness of shaving combined with compression in the
treatment of Elephantiasis Nostras Verrucosa in advanced primary lymphedema,
analyzing clinical results and recurrence at five years.
|
A
retrospective, descriptive, and quantitative study, complemented by a
literature review on the topic.
|
The
treatment significantly reduced episodes of erysipelas, eliminated recurrence
of Elephantiasis Nostras Verrucosa (ENV), and improved limb function. The
combination of shaving, compression, and liposuction proved effective in
functional and aesthetic rehabilitation.
|
|
Antibacterial activity of methanol
extracts
of the leaves of three medicinal plants
against selected bacteria isolated from
wounds of
lymphoedema patients.21
|
Ethiopia
/2021
|
To
investigate the antibacterial activity of methanolic extracts of Lawsonia
inermis, Azadirachta indica, and Achyranthes aspera leaves against bacteria
isolated from wounds in patients with lymphedema.
|
Experimental
and descriptive study, conducted in a laboratory.
|
Lawsonia
inermis demonstrated the highest antibacterial activity against all strains
tested, while Azadirachta indica showed a moderate effect and Achyranthes
aspera low efficacy.
|
|
Primary lymphedema French National
Diagnosis and Care Protocol (PNDS;
Protocole
National de
Diagnostic et de Soins).18
|
France/
2021
|
To
establish national guidelines for the diagnosis, monitoring, and treatment of
primary lymphedema in France.
|
This is a
descriptive, qualitative, and guideline-review study, including a narrative
literature review and analysis of existing protocols.
|
It
established clinical and genetic diagnostic criteria, recommended imaging
tests, and standardized treatment with decongestive therapy, compression, and
a multidisciplinary approach.
|
|
Dermo-Hipodermites Bacterianas Agudas
Não
Necrotizantes:
Erisipela e Celulite Infeciosa.17
|
Portugal/
2021
|
Describe the
clinical aspects, risk factors, diagnosis, and treatment of erysipelas and
infectious cellulitis.
|
This is a
descriptive and qualitative study, a narrative literature review, based on
published clinical and microbiological evidence on erysipelas and cellulitis.
|
Infections
caused by Streptococcus pyogenes affect the lower limbs. Diagnosis is
clinical, and antibiotic treatment reduces recurrences; benzathine penicillin
is effective in prevention.
|
|
Liposuction and Controlled Compression
Therapy
Reduce the Erysipelas Incidence in
Primary and
Secondary
Lymphedema.12
|
Sweden/
2022
|
To evaluate
the impact of liposuction combined with controlled compression therapy in
reducing the incidence of erysipelas in patients with primary and secondary
lymphedema.
|
This was a
retrospective, observational, and quantitative study conducted with patients
who underwent liposuction followed by continuous compression therapy.
|
There was
a significant reduction in erysipelas with the combined therapy. Controlled
compression was essential to prevent recurrence and maintain reduced
lymphatic volume.
|
|
The VASCERN PPL working group patient
pathway for primary and
paediatric
lymphoedema.19
|
Europe:
France, United Kingdom, Belgium, Italy and Sweden / 2024
|
To
standardize the care pathway for diagnosis, treatment, and follow-up of
primary and pediatric lymphedema in Europe, promoting uniformity of care
among specialized centers.
|
This is a
descriptive and qualitative study, of the expert opinion/consensus type;
based on a narrative literature review, existing protocols, and clinical
experience of the centers that are part of the VASCERN PPL network.
|
It
established a patient care flow with diagnostic steps, imaging exams, and
treatment based on decongestive therapy, compression, and a multidisciplinary
approach among European centers.
|
|
Swelling of
the legs and feet.14
|
UK/
2025
|
To review
the main causes of lower limb edema and present current diagnostic and
therapeutic approaches, with emphasis on the most common conditions in adults
in the Western world.
|
A descriptive
and qualitative literature review, based on scientific publications and
clinical guidelines on the causes, diagnosis, and treatment of edema in the
lower limbs.
|
The main
findings show that chronic venous insufficiency, lymphedema, and lipedema are
the most common causes of leg swelling. Early treatment with compression
therapy, skin care, and patient education is essential to prevent
complications and improve quality of life.
|
Source:
The authors, 2025.
In summary, the findings highlight
important advances in combined therapies and the consolidation of international
clinical protocols, although there remains a need for greater participation
from nursing-led studies, especially in the contexts of prevention,
rehabilitation, and follow-up of patients with lymphedema associated with
erysipelas.
DISCUSSION
To provide a better analysis of the following results in
the discussion, it was necessary to develop three sections: 1. Therapeutic
approaches and clinical efficacy in the management of lymphedema associated
with erysipelas; 2. Clinical protocols, standardization, and the role of
nursing in multidisciplinary care; 3. Therapeutic innovations and integrative
perspectives in the treatment of cutaneous and bullous lesions.
1. Therapeutic approaches and clinical efficacy in the
management of lymphedema associated with erysipelas
The evaluation of scientific indicators
demonstrates that therapeutic approaches aimed at managing lymphedema in
patients with erysipelas are confirmed through combined therapies, which relate
pharmacological control, surgical intervention, and physiotherapeutic support.
The study of the effectiveness of the association between liposuction and
controlled compression therapy in reducing the incidence of erysipelas in
patients with primary and secondary lymphedema proved promising. This treatment
has proven effective in reducing lymphatic volume, as well as in preventing
relapses, reflecting a considerable advance in terms of quality of life and
functional recovery of affected patients(12).
In addition, the shaving technique
combined with continuous compression, used in cases of Elephantiasis Nostras
Verrucosa, a critical manifestation of advanced lymphedema, reveals promising
effects. Therefore, the therapeutic combination eliminated recurrent cases of
infection and improved motor function of the lower limbs, indicating that
aesthetic and functional rehabilitation depends on the application of
integrated and continuous protocols of compression and lymphatic drainage.
Concomitantly, the evidence in question strengthens the need for
multidisciplinary care, highlighting the role of the nurse in preventing
infectious relapses and assisting in treatment aadherenc(13).
Contributing to this thinking, a
multidisciplinary approach is recommended, involving a specialized lymphatic
nurse, physiotherapist, clinical geneticist, vascular specialist, and
psychologist. Traditional measures, also known as decongestive lymphatic therapy
or lymphatic decongestion therapy, protect the skin and open collateral
lymphatic drainage. These methods include graduated compression stockings (GC),
as they reduce capillary absorption and contribute to the calf muscle pump,
reducing interstitial lymphatic fluid. Intermittent pneumatic compression, with
pressures up to 150 mmHg, has proven effective in reducing lower limb
lymphedema, especially in bedridden patients or those with reduced mobility.
Furthermore, maintaining compression therapy for a long period of time using
graduated compression stockings or inelastic bandages is also essential(14).
Therefore, it is emphasized that the
use of benzopyrones, when related to complex decongestive therapy, shows good
results in the treatment of lymphedema. However, these medications are not yet
approved for prescription in many countries. Furthermore, it reinforces the
importance of recognizing and treating episodes of erysipelas and lymphangitis
quickly, since early therapy can prevent serious complications such as sepsis
or even total limb loss during the acute phase of the disease. In cases with a
high amount of exudate, it is advisable to start treatment with bandages in the
first few weeks. After this period, these bandages can be used over Zetuvit
Plus (Paul Hartmann Ltd, Heywood, UK), which are thin, absorbent dressings,
especially when erysipelas causes skin llesion(14).
Despite surgical interventions, the
literature emphasizes the use of substances with antioxidant and
anti-inflammatory properties as therapeutic adjuvants. Following this line of
thought, a study analyzed the efficacy of sodium selenite in patients with cancer-associated
lymphedema and found a significant reduction in edema, local inflammation, and
the frequency of recurrent erysipelas. Selenite enhances the response to
physiotherapy treatment and potentiates cellular oxidative metabolism, which,
upon analysis, may be relevant for patients suffering from chronic erysipelas
and skin lesions that are difficult to heal(15).
Furthermore, in the area of
antibiotic pharmacotherapy, the S2k guidelines implement safe protocols for the
treatment of bacterial skin infections, such as erysipelas and infectious
cellulitis. The conscious use of penicillin and cephalosporins is reflected as
a first-line plan, while severe cases require broad-spectrum antibiotics or
complementary surgical interventions. Following this line of thought, these
guidelines are fundamental to reducing bacterial resistance and guiding
standardized clinical management(16).
Erysipelas is characterized by the
unexpected onset of fever, specifically between 38.5°C and 40°C, manifesting as
bright red, warm, erythematous plaques accompanied by pain. Furthermore, skin
lesions may appear, measuring approximately 10 to 15 cm in their largest area,
and are accompanied by flaccid, bullous vesicles with a translucent interior.
In this context, for most patients, empirical coverage against
methicillin-sensitive Staphylococcus aureus (MSSA) and streptococci is
sufficient. Flucloxacillin and first-generation cephalosporins, such as
cefradine, are chosen as first-line treatments due to their efficacy and
appropriate size. In patients allergic to penicillin, clarithromycin or
clindamycin are suitable options. Generally, a seven-day treatment period is
sufficient, with improvement in fever and pain within 24–48 hours and complete
resolution of skin signs within two weeks. In bullous cases, such as bullous
erysipelas, re-epithelialization can extend for about 20 days(17).
In contrast, coverage for
methicillin-resistant Staphylococcus aureus (MRSA) should be reserved for
specific occasions, such as traumatic wounds, a previous history of MRSA, or
intravenous drug use. In these cases, oral therapy can be established with the
addition of cotrimoxazole or doxycycline to the beta-lactam, or by replacing it
with clindamycin(17).
Patients meeting hospitalization
criteria should receive intravenous antibiotic therapy, with flucloxacillin or
cefazolin being the initial indications. Patients allergic to penicillin can
use clarithromycin or clindamycin. In a hospital setting with suspected MRSA,
vancomycin is advised, with linezolid as an alternative measure. Therefore,
Chart 3 presents the most effective antibiotic therapies with their respective
dosages(17).
Chart 3 -
Antibiotic regimen for the treatment of erysipelas.
|
Clinical Scenario
|
Therapeutic options
|
Penicillin Allergy
|
|
Outpatient clinic l
|
•
Flucloxacillin - 500mg every 6 hours (orally);
•
Cefradine - 500mg every 6 hours (orally);
•
Amoxicillin/Clavulanic Acid - 875mg + 125mg every 12 hours (orally);
•
Clindamycin - 300mg every 6 hours (orally);
•
Ciprofloxacin - 750mg every 12 hours (orally);
|
•Clarithromycin
500 mg every 12 hours (orally);
•Clindamycin
600 mg every 8 hours (orally);
|
|
Hospitalization
|
•
Flucloxacillin - 2g every 6 hours (IV);
•
Cephaloxine 1g every 6 hours (IV);
•
Amoxicillin/Clavulanic Acid - 1000 mg + 100 mg every 12 hours (PO);
•
Imipenem 1-2g every 8 hours (IV);
|
•
Clarithromycin - 500mg every 12 hours (IV);
•
Clindamycin - 900mg every 8 hours (IV);
|
|
Suspected or confirmed case of MRSA.
|
•
Vancomycin 1-2g/day (IV);
•
Linezolid (dose according to clinical protocol);
|
---------------------------------
|
Source: Adapted from Rodrigues, 2021.
In addition to these, antibiotic
prevention has also proven effective in preventing relapses in patients with
two or more episodes of lymphedema associated with erysipelas, using benzathine
penicillin 1.2–2.4 million units every 4 weeks intramuscularly or erythromycin
250 mg/day in episodes of penicillin allergy. This measure reduces the risk of
relapses during treatment by about 70%, even though its effect is only
suppressive. Obese patients with a Body Mass Index (BMI ≥ 33), with multiple
relapses or lymphedema, show a lower response to prophylaxis(17).
Furthermore, the agreement between
surgical, compressive, and pharmacological therapies reaffirms that the
treatment of lymphedema associated with erysipelas should not be separate, but
integrated into an interdisciplinary approach. In this way, the nurse plays a
central role in this process, that is, acting in monitoring, therapeutic
adherence and infection control in health services, as well as acting in health
education, wound care and rehabilitation, ensuring that therapeutic measures
are effective, consistent and sustainable(17).
2. Clinical protocols, standardization and the role of nursing in
multidisciplinary care
International guidelines have adopted a
fundamental role in standardizing clinical conduct in the face of lymphedema
and its infectious complications. The French National Diagnosis and Care
Protocol (PNDS) proposes an integrated care structure that guides from
diagnosis to rehabilitation. The protocol highlights the use of combined
decongestive therapy, manual lymphatic drainage, elastic compression and skin
care as essential pillars of treatment. Additionally, it emphasizes the
importance of a multidisciplinary approach, which includes physicians,
physiotherapists, psychologists and nurses trained in the management of
lymphedema and recurrent skin infections(18).
In this context, the European working
group VASCERN PPL developed a patient pathway for primary and pediatric
lymphedema. This model, in addition to standardizing diagnostic steps and
imaging exams, establishes longitudinal follow-up of patients, ensuring
continuity of care and equity in treatments among different European countries.
This approach highlights the importance of referral centers and the coordinated
action of nursing professionals in clinical surveillance and guidance on
self-care, preventing complications such as bullous and ulcerated lesions
resulting from erysipelas(19).
The diagnosis of lymphedema is
primarily clinical and should be confirmed by integrated imaging methods, such
as lymphoscintigraphy and ultrasound. Appropriate practice includes
decongestive therapy measures, compression, and daily skin care, with surgical
intervention indicated only in resistant cases. This conservative management is
what most favors adherence and maintenance of skin integrity, demonstrating the
importance of constant monitoring by nursing staff, who act directly in the
prevention of lesions and the early identification of infectious signs(20).
In addition, it is noteworthy that
erysipelas is an infection that continuously affects the lower limbs and can be
recurrent in patients with lymphedema. Therefore, it is emphasized that early
diagnosis and treatment with benzathine penicillin are crucial to reduce
relapses, considering the importance of care protocols that prioritize
antibiotic prophylaxis and comprehensive care(17).
Thus, it is observed that the
consolidation of clinical protocols, such as the PNDS, the VASCERN PPL, and the
S2k guidelines, contribute to the centralization of practices and the
improvement of the quality of care. These protocols provide support for nursing
to act autonomously and based on evidence, corroborating its contribution in
the stages of assessment, treatment, and follow-up of patients with lymphedema
and erysipelas (18,19,16).
3.
Therapeutic innovations and integrative perspectives in the treatment of
cutaneous and bullous lesions.
The
growth of experimental research has generated new concepts for the treatment of
lymphedema associated with cutaneous and bullous lesions. Therefore, the
therapeutic potential of methanolic extracts of medicinal plants, such as Lawsonia
inermis and Azadirachta indica, is highlighted. These plants showed
significant antibacterial activity against microorganisms specific to wounds in
patients with lymphedema. In this sense, the methanolic extract of L.
inermis (Henna) presented the highest yield of bioactive compounds (15.9%)
and validated the most significant antibacterial and bactericidal action among
the plants tested. Inhibition halos comparable to those produced by reference
antibiotics (cefoxitin and penicillin) were analyzed, particularly against strains
of Staphylococcus aureus and Streptococcus pyogenes, determinants
of erysipelas and secondary infections in lymphedema. The high efficacy of L.
inermis is related to the presence of anthraquinones, phenols, flavonoids, and
tannins, compounds characterized by their antimicrobial, antioxidant, and
healing action(21).
Regarding the methanolic extract of
Achyranthes aspera (Telenge), it revealed an intermediate yield (14.7%) and a
more limited antibacterial activity, but still efficient against Streptococcus
pyogenes, a pathogen strongly linked to occurrences of recurrent erysipelas.
Its phytochemical composition showed the presence of alkaloids, tannins, and
terpenoids, compounds that have moderate antimicrobial and anti-inflammatory
properties. Even less potent than L. inermis, this A. aspera extract can act
synergistically when integrated with other natural agents, helping to maintain
control of the microbial load and reduce inflammation in affected tissues(21).
Furthermore, regarding the methanolic
extract of Azadirachta indica (Neem), it showed a yield of 7.9%, with moderate
but consistent antibacterial activity against Gram-positive microorganisms,
including S. pyogenes and S. aureus. Its function is related to the presence of
flavonoids, terpenoids, and saponins, compounds known to have
anti-inflammatory, bacteriostatic, and immunomodulatory effects. In the context
of lymphedema and erysipelas wounds, these effects are especially important, as
they reduce excessive inflammatory response, local edema, and help prevent
recurrent bacterial reinfections(21).
Therefore, even though A. aspera has
a higher yield, its antibacterial efficiency is less pronounced compared to A.
indica, even with a lower yield, because its composition is more concentrated
in bioactive compounds such as flavonoids, terpenoids, and saponins. These
findings reflect an important advance in the development of alternative or
complementary therapies, especially in regions with limited access to
conventional antibiotics. Another relevant aspect is reinforcing the
possibility of integrating herbal medicines into safe clinical protocols,
provided they are validated by controlled trials and guided by qualified
healthcare professionals. However, safe therapeutic implementation requires
supplementary clinical studies to evaluate ideal concentrations for topical
use, potential adverse effects, and the standardization of plant extracts(21).
In line with this, in addition to
antibiotic therapy and medicinal means, it is essential to adopt general care
methods, such as rest with elevation of the affected limb, careful puncture of
blisters without removing the top layer of the blister, avoiding the use of
irritating antiseptics, thus promoting skin re-epithelialization. In bullous
cases, the application of topical antibiotics may be necessary, such as 2%
fusidic acid, 20 mg/g mupirocin, or 1% silver sulfadiazine. Thus, nursing plays
a prominent role in monitoring the use of antimicrobials and implementing safe
care practices, providing therapeutic adherence and preventing new lesions(17).
The combination of surgical
interventions and compression therapies can provide not only edema reduction
but also tissue regeneration, improving skin texture and lymphatic function.
This innovative approach is combined with integrative rehabilitation strategies
that value the aesthetics and psychosocial well-being of the patient. These
dimensions are fundamental, since lymphedema and bullous lesions significantly
impact self-esteem and body image, factors that require sensitivity from the
nursing team during care and guidance(13).
Beyond pharmacological and surgical
innovations, there is a growing appreciation for educational and preventive
measures aimed at reducing risk factors and early detection of skin lesions.
The PNDS and VASCERN PPL indicate that patient empowerment and self-care
monitored by nursing staff are essential means for therapeutic success(18-19).
Therefore, these practices include guidance on local hygiene, weight control,
management of skin trauma, and the continuous use of compression stockings,
measures that decrease the possibility of erysipelas recurrence and delay the
progression of lymphedema.
Given the above, it is pertinent to
acknowledge the limitations and strengths of this study. Among the limitations,
the lack of studies focused on the role of nursing in the management of
lymphedema related to erysipelas stands out, which reduces the detailed
analysis of clinical practices and care strategies developed by the category.
Furthermore, the inclusion of review
studies in the sample was noted as important, since the production of primary
research on the topic is still small. This measure was essential to increase
theoretical understanding and gather sufficient evidence to allow for a
comprehensive and well-founded discussion of the topic.
On the other hand, this study reveals
strengths, such as the robust search in scientific databases, which allowed for
a careful and up-to-date selection of available evidence. Added to this is the
novelty of the proposal, which systematically unites therapeutic,
pharmacological, and care approaches related to lymphedema and erysipelas from
a nursing perspective. The importance of the topic is also highlighted, as it
contributes to strengthening interdisciplinary care, improving clinical
practice, and valuing the role of nurses in the prevention and management of
cutaneous and bullous complications resulting from these conditions.
Therefore, it is evident that the
most recent evidence converges on the importance of more patient-centered care,
focusing on appropriate therapies and interdisciplinary support. The nurse
emerges as an essential professional in integrating clinical treatment,
psychological support, and self-care practices, acting as a mediator between
medical actions and the individual needs of the patient. Therefore, the
treatment of lymphedema related to erysipelas should be understood as an
ongoing process that connects science, humanization, and technological
innovation.
FINAL CONSIDERATIONS
The findings of this review highlighted
that the treatment of lymphedema associated with the development of cutaneous
and bullous lesions in patients with erysipelas requires a comprehensive
approach, supported by combined therapeutic practices. The therapeutic measures
analyzed demonstrated consistent results in reducing edema, preventing
relapses, controlling skin infections, and maintaining skin integrity,
especially when associated with continuous compression interventions, manual
lymphatic drainage, specific surgical therapies, and the use of pharmacological
agents.
International clinical protocols have
also proven to be extremely important for standardizing management, improving
early diagnosis, and guiding long-term care strategies. However, the lack of
scientific publications related to nursing practice is emphasized, especially
regarding the prevention, rehabilitation, and follow-up of patients with
lymphedema associated with erysipelas. The increase in primary research
focusing on clinical and educational care is extremely relevant to promote
professional practice and improve evidence-based conduct. Despite this
limitation, this review highlights the systematization of updated studies,
which offer theoretical and practical support to improve care.
Based on this evidence, it becomes
clear that managing these conditions requires interdisciplinary actions,
therapeutic continuity, and effective health education. Nurses occupy an
essential position in this process, acting in clinical surveillance, treatment
monitoring, wound care, and guidance on self-care. Therefore, the treatment of
lymphedema associated with erysipelas should be understood as constant care
that combines science, technology, and humanization, seeking to reduce
complications, promote autonomy, and improve the quality of life of patients.
REFERENCES
1. Araújo RC,
Alexandrino A, Sousa ATO. Erisipela e celulite: diagnóstico, tratamento e
cuidados gerais. Ver Enferm Atual In Derme. 2021;95(36).
Doi:10.31011/reaid-2021-v.95- n.36-art.1240.
2.
Giroto
CP, Rocha MESB, Pinto NNS, Lima RC, Chikui BYO, Souza GL, et al. Erisipela:
explorando a contaminação e a incidência de lesões causadas por infecção
bacteriana. Braz J Implant Health Sci. 2024;6(1):17-28. doi:10.36557/2674-8169.2024v6n1p17-28.
3.
Caetano M, Amorin I. Erisipela. Acta Med Port.
2005;18(5):385-393. doi:10.20344/amp.1040.
4.
Pearce
J, Gordon K, Mortimer P. Vascularand lymphatic abnormalities. Dermatology and
general health. 2025;53(8):494-496. doi:10.1016/j.mpmed.2025.05.001.
5.
Barajas-Puga
JÁ, Soto-Verdugo LA, González-Godínez C, Zamora-Inzunza JG, Tirado- Peraza ÁI.
Manejo quirúrgico del linfedema. Cir Plast. 2023;33(4):187-194. doi:10.35366/113886.
6. Meneses AB,
Rodrigues CSS, Sousa MSC, Castilho JC, Oliveira PG. Tratamento de lesões
decorrentes de processo infeccioso por erisipela: relato de experiência. Rev
Feridas. 2019;7(39):1406-1413. doi:10.36489/feridas.2019v7i39p1406-1413.
7. Gomes A.
Erisipela: causas e tratamento. Rev Feridas. 2019;7(37):1322-1324. doi:10.36489/feridas.2019v7i37p1322-1324.
8.
Rosaneli
CF, Fischer ML. A revisão integrativa como ferramenta para educação
profissional e tecnológica em Bioética. Revista Brasileira da Educação
Profissional e Tecnológica. 2024. doi:10.15628/rbept.2024.17809.
9.
Van der Waldt G. Formulating research questions in social science
research. J Transdiscipl Res South Afr. 2025;21(1):a1526.
Doi:10.4102/td.v21i1.1526.
10. Costa ICP, Mendes
KDS, Freitas PS. Estratégias de busca na literatura: roteiro para identificação
das melhores evidências na área da saúde. Texto Contexto Enferm.
2025;34:e20230405. doi:10.1590/1980-265X-TCE-2023-0405pt.
11.
Page
MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The
PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
doi:10.1136/bmj.n71.
12.
Karlsson T, Hoffner M, Brorson H. Liposuction and controlled compression therapy reduce the
erysipelas incidence in primary and secondary lymphedema. Plast Reconstr
Surg Glob Open. 2022;10(5):e4314. doi:10.1097/GOX.0000000000004314.
13. Damstra RJ, Dickinson-Blok JL, Voesten HG. Shaving technique and compression therapy for elephantiasis nostras verrucosa of forefeet and toes in end-stage primary
lymphedema: a 5- year follow-up study. J Clin Med.
2020;9(10):3139. doi:10.3390/jcm9103139.
14. Govender D, Howard AQ. Swelling of the legs and feet.
Surgery (Oxford). 2025;43(5):286-298.
doi:10.1016/j.mpsur.2025.03.008.
15. Pfister C,
Dawczynski H, Schingale FJ. Sodium selenite and cancer-related lymphedema:
biological and pharmacological effects. J Trace Elem Med Biol. 2016;37:111-116. doi:10.1016/j.jtemb.2016.05.005.
16. Sunderkötter C, Becker K, Eckmann C, Graninger W, Kujath P, Schöfer H. S2k guidelines for skin and soft tissue
infections: excerpts from the S2k guidelines for calculated initial parenteral treatment
of bacterial infections
in adults. J Dtsch Dermatol
Ges. 2019;17(3):345-369. doi:10.1111/ddg.13790.
17. Rodrigues MA, Caetano M, Amorim I, Selores M. Dermo-hipodermites bacterianas agudas não necrotizantes: erisipela e celulite infecciosa. Acta
Med Port. 2021;34(3):217-228. doi:10.20344/amp.12642.
18. Vignes
S, Albuisson J, Champion L, Constans J, Tauveron V, Malloizel J, et al. Primary
lymphedema French national
diagnosis and care protocol. Orphanet
J Rare Dis. 2021;16(1):18. doi:10.1186/s13023-020-01652-w.
19.
Devoogdt
N, Thomis S, Belva F, Dickinson-Blok J, Fourgeaud C, Giacalone G, et al. The
VASCERN PPL working group patient
pathway for primary
and paediatric lymphoedema. Eur
J Med Genet. 2024;67:104905. doi:10.1016/j.ejmg.2023.104905.
20. Grada
AA, Phillips TJ. Lymphedema: diagnostic workup and management. J Am Acad
Dermatol. 2017;77(6):995-1006. doi:10.1016/j.jaad.2017.03.021.
21. Nigussie D, Belew
S, Alemayehu M, Abate E, Ali J, Demeke G. Antibacterial activity of methanol
extracts of the leaves of medicinal plants against bacteria isolated from
wounds of lymphedema patients. BMC Complement Med Ther. 2021;21(1):2.
doi:10.1186/s12906-020- 03183-0.
Funding and Acknowledgments:
This research received no funding.
Conflict of Interest Statement
“Nothing to declare.”
Data Availability Statement
No databases were generated in this study. The
information presented is described in the body of the article.
Authorship Criteria (Author Contributions)
Authorship designation should be based on
ICMJE guidelines, which consider an author to be someone who: 1. contributes
substantially to the conception and/or planning of the study; 2. to the
acquisition, analysis, and/or interpretation of the data; 3. as well as to the
drafting and/or critical revision and final approval of the published version.
Larissa Fernandes da Silva Oliveira: 1,2,3
Melka Maria Frazão de Souza:1,2,3
Paulo Geovane Pestana Pinheiro: 1,2,3
Francisco Carlos Costa Magalhães: 1,2,3
Mayra Sharlenne Moraes Araújo: 1,2,3
Tamires Barradas Cavalcante: 1,2,3
Scientific Editor: Ítalo
Arão Pereira Ribeiro. Orcid: https://orcid.org/0000-0003-0778-1447
Rev Enferm Atual In Derme 2026;100(2):
e026039